MarylandQuitter
-
Posts
3701 -
Joined
-
Last visited
-
Days Won
15
Content Type
Profiles
Forums
Events
Blogs
Gallery
Everything posted by MarylandQuitter
-
 February 4, 2019 Stanton A. Glantz, PhD https://tobacco.ucsf.edu/rct-comparing-e-cigs-nrt-shows-effectiveness-supervised-smoking-cessation-program-what-it-does-and-does-not-mean?fbclid=IwAR3BTV8SJ13deT_tMOiQFOhcidWO1jEkakN-ynQbJtIxNJ4gprzkn0OMZvY RCT comparing e-cigs to NRT shows effectiveness in a supervised smoking cessation program: what it does and does not mean February 4, 2019 Stanton A. Glantz, PhD RCT comparing e-cigs to NRT shows effectiveness in a supervised smoking cessation program: what it does and does not mean Peter Hajek and colleagues published “A Randomized Trial of E-cigarettes versus Nicotine-Replacement Therapy” in the New England Journal of Medicine. This is a well-done trial comparing e-cigarettes with nicotine replacement therapy among people enrolled in smoking cessation programs in England. In addition to being randomized to e-cigs or NRT, people in the study had at least 4 weeks of counseling. At one year the cigarette abstinence rate was 18.0% among patients randomized to e-cigs compared to 9.9% randomized to NRT, nearly a doubling of quitting. The study is thoughtfully designed and cautiously interpreted. The authors also did a nice set of sensitivity analyses to show that the results are robust to the usual kinds of problems one has in doing a randomized controlled trial. They conclude that “E-cigarettes were more effective for smoking cessation that nicotine-replacement therapy, when both products were accompanied by behavioral support.” I agree with that conclusion. Having said that, it is important to emphasize that this is not a study of e-cigarettes as most people use them, which is as recreational products not as part of a clinically supervised cessation attempt that, most important, includes intensive counseling. Thus, the results of the Hajek study do not contradict the overall result that, in the general population, smokers who use e-cigarettes are, on average, less likely to quit smoking. So, my bottom line is that if other well-done randomized controlled trials show that e-cigarettes improve smoking cessation, the manufacturers should submit the evidence to the appropriate authorities (the FDA in the USA) to get e-cigarettes approved as prescription medicines to be administered by physicians or other health professionals as part of supervised cessation efforts that include intensive counseling. The reason that I say they should be available by prescription is because of their high abuse potential, as evidenced by the run-away use of them by kids as well as the fact that when used unsupervised in the general population they depress smoking cessation. In addition to efficacy, the drug approval process needs to assess safety. Hajek and colleagues reported that after one year 80% of the e-cigarette group were still using e-cigarettes compared to just 9% of the NRT group were continuing to use NRT. This is of particular concern because of the evidence linking e-cigarette use to heart attacks and chronic obstructive pulmonary disease and is something that warrants serious consideration by regulatory authorities. The accompanying editorial by Belinda Borrelli and George T. O’Connor also raises several concerns about long-term safety of e-cigarette use and notes that varenicline -- which was not evaluated in the Hajek study -- outperforms NRT. Here is the abstract: BACKGROUND: E-cigarettes are commonly used in attempts to stop smoking, but evidence is limited regarding their effectiveness as compared with that of nicotine products approved as smoking-cessation treatments. METHODS: We randomly assigned adults attending U.K. National Health Service stop-smoking services to either nicotine-replacement products of their choice, including product combinations, provided for up to 3 months, or an e-cigarette starter pack (a second-generation refillable e-cigarette with one bottle of nicotine e-liquid [18 mg per milliliter]), with a recommendation to purchase further e-liquids of the flavor and strength of their choice. Treatment included weekly behavioral support for at least 4 weeks. The primary outcome was sustained abstinence for 1 year, which was validated biochemically at the final visit. Participants who were lost to follow-up or did not provide biochemical validation were considered to not be abstinent. Secondary outcomes included participant-reported treatment usage and respiratory symptoms. RESULTS: A total of 886 participants underwent randomization. The 1-year abstinence rate was 18.0% in the e-cigarette group, as compared with 9.9% in the nicotine-replacement group (relative risk, 1.83; 95% confidence interval [CI], 1.30 to 2.58; P<0.001). Among participants with 1-year abstinence, those in the e-cigarette group were more likely than those in the nicotine-replacement group to use their assigned product at 52 weeks (80% [63 of 79 participants] vs. 9% [4 of 44 participants]). Overall, throat or mouth irritation was reported more frequently in the e-cigarette group (65.3%, vs. 51.2% in the nicotine-replacement group) and nausea more frequently in the nicotine-replacement group (37.9%, vs. 31.3% in the e-cigarette group). The e-cigarette group reported greater declines in the incidence of cough and phlegm production from baseline to 52 weeks than did the nicotine-replacement group (relative risk for cough, 0.8; 95% CI, 0.6 to 0.9; relative risk for phlegm, 0.7; 95% CI, 0.6 to 0.9). There were no significant between-group differences in the incidence of wheezing or shortness of breath. CONCLUSIONS: E-cigarettes were more effective for smoking cessation than nicotine-replacement therapy, when both products were accompanied by behavioral support. (Funded by the National Institute for Health Research and Cancer Research UK; Current Controlled Trials number, ISRCTN60477608 .). The full citation is Hajek P, et al. A Randomized Trial of E-Cigarettes versus Nicotine-Replacement Therapy. N Engl J Med. 2019 Jan 30. doi: 10.1056/NEJMoa1808779. [Epub ahead of print]. The paper is available here.
February 4, 2019 Stanton A. Glantz, PhD https://tobacco.ucsf.edu/rct-comparing-e-cigs-nrt-shows-effectiveness-supervised-smoking-cessation-program-what-it-does-and-does-not-mean?fbclid=IwAR3BTV8SJ13deT_tMOiQFOhcidWO1jEkakN-ynQbJtIxNJ4gprzkn0OMZvY RCT comparing e-cigs to NRT shows effectiveness in a supervised smoking cessation program: what it does and does not mean February 4, 2019 Stanton A. Glantz, PhD RCT comparing e-cigs to NRT shows effectiveness in a supervised smoking cessation program: what it does and does not mean Peter Hajek and colleagues published “A Randomized Trial of E-cigarettes versus Nicotine-Replacement Therapy” in the New England Journal of Medicine. This is a well-done trial comparing e-cigarettes with nicotine replacement therapy among people enrolled in smoking cessation programs in England. In addition to being randomized to e-cigs or NRT, people in the study had at least 4 weeks of counseling. At one year the cigarette abstinence rate was 18.0% among patients randomized to e-cigs compared to 9.9% randomized to NRT, nearly a doubling of quitting. The study is thoughtfully designed and cautiously interpreted. The authors also did a nice set of sensitivity analyses to show that the results are robust to the usual kinds of problems one has in doing a randomized controlled trial. They conclude that “E-cigarettes were more effective for smoking cessation that nicotine-replacement therapy, when both products were accompanied by behavioral support.” I agree with that conclusion. Having said that, it is important to emphasize that this is not a study of e-cigarettes as most people use them, which is as recreational products not as part of a clinically supervised cessation attempt that, most important, includes intensive counseling. Thus, the results of the Hajek study do not contradict the overall result that, in the general population, smokers who use e-cigarettes are, on average, less likely to quit smoking. So, my bottom line is that if other well-done randomized controlled trials show that e-cigarettes improve smoking cessation, the manufacturers should submit the evidence to the appropriate authorities (the FDA in the USA) to get e-cigarettes approved as prescription medicines to be administered by physicians or other health professionals as part of supervised cessation efforts that include intensive counseling. The reason that I say they should be available by prescription is because of their high abuse potential, as evidenced by the run-away use of them by kids as well as the fact that when used unsupervised in the general population they depress smoking cessation. In addition to efficacy, the drug approval process needs to assess safety. Hajek and colleagues reported that after one year 80% of the e-cigarette group were still using e-cigarettes compared to just 9% of the NRT group were continuing to use NRT. This is of particular concern because of the evidence linking e-cigarette use to heart attacks and chronic obstructive pulmonary disease and is something that warrants serious consideration by regulatory authorities. The accompanying editorial by Belinda Borrelli and George T. O’Connor also raises several concerns about long-term safety of e-cigarette use and notes that varenicline -- which was not evaluated in the Hajek study -- outperforms NRT. Here is the abstract: BACKGROUND: E-cigarettes are commonly used in attempts to stop smoking, but evidence is limited regarding their effectiveness as compared with that of nicotine products approved as smoking-cessation treatments. METHODS: We randomly assigned adults attending U.K. National Health Service stop-smoking services to either nicotine-replacement products of their choice, including product combinations, provided for up to 3 months, or an e-cigarette starter pack (a second-generation refillable e-cigarette with one bottle of nicotine e-liquid [18 mg per milliliter]), with a recommendation to purchase further e-liquids of the flavor and strength of their choice. Treatment included weekly behavioral support for at least 4 weeks. The primary outcome was sustained abstinence for 1 year, which was validated biochemically at the final visit. Participants who were lost to follow-up or did not provide biochemical validation were considered to not be abstinent. Secondary outcomes included participant-reported treatment usage and respiratory symptoms. RESULTS: A total of 886 participants underwent randomization. The 1-year abstinence rate was 18.0% in the e-cigarette group, as compared with 9.9% in the nicotine-replacement group (relative risk, 1.83; 95% confidence interval [CI], 1.30 to 2.58; P<0.001). Among participants with 1-year abstinence, those in the e-cigarette group were more likely than those in the nicotine-replacement group to use their assigned product at 52 weeks (80% [63 of 79 participants] vs. 9% [4 of 44 participants]). Overall, throat or mouth irritation was reported more frequently in the e-cigarette group (65.3%, vs. 51.2% in the nicotine-replacement group) and nausea more frequently in the nicotine-replacement group (37.9%, vs. 31.3% in the e-cigarette group). The e-cigarette group reported greater declines in the incidence of cough and phlegm production from baseline to 52 weeks than did the nicotine-replacement group (relative risk for cough, 0.8; 95% CI, 0.6 to 0.9; relative risk for phlegm, 0.7; 95% CI, 0.6 to 0.9). There were no significant between-group differences in the incidence of wheezing or shortness of breath. CONCLUSIONS: E-cigarettes were more effective for smoking cessation than nicotine-replacement therapy, when both products were accompanied by behavioral support. (Funded by the National Institute for Health Research and Cancer Research UK; Current Controlled Trials number, ISRCTN60477608 .). The full citation is Hajek P, et al. A Randomized Trial of E-Cigarettes versus Nicotine-Replacement Therapy. N Engl J Med. 2019 Jan 30. doi: 10.1056/NEJMoa1808779. [Epub ahead of print]. The paper is available here. -
February 5, 2019 Stanton A. Glantz, PhD Another study ties e-cigs to strokes and confirms association with heart attacks https://tobacco.ucsf.edu/another-study-ties-e-cigs-strokes-and-confirms-association-heart-attacks?fbclid=IwAR2aK6T2Gkvb6wVPo8gJyahJt9Eqg8cna0T6xzaWatoNTxtTxskVoxPGc-8 Paul M Ndunda and Tabitha M Muutu just presented their paper “Electronic Cigarette Use is Associated With a Higher Risk of Stroke” at the International Stroke Conference. They conducted a cross-sectional analysis using the CDC’s Behavorial Risk Factor Surveillance System data from 2016 to assess the risks of stroke and myocardial infarction in e-cigarette users, controlling for cigarette smoking. They found compared with non-users, e-cigarette users had higher adjusted odds of stroke (OR 1.71 [1.64 - 1.8]), myocardial infarction (OR 1.59 [1.53 - 1.66]), angina or coronary heart disease (OR 1.4 [1.35 - 1.46]). These risks are similar to what we reported based on the National Health Interview Survey. The fact that two independent data sources yielded such similar results is strong evidence that the association is real. Farsalinos has already criticized the paper, mostly with linguistic challenges of what the word “risk factor” means. Had he checked Wikipedia he would have seen that the term “risk factor” is meant to be used when describing associations in cross-sectional studies. Here is an NPR story on the study that has a good description and puts it into context.
-
Feb 05 2019 An exploding vaporiser pen resulted in the death of a 24-year-old Texas man, a post-mortem examination has ruled. https://www.bbc.com/news/world-us-canada-47136678 The pen's battery blew up when William Brown tried to use it, sending shards of metal into his face and neck and severing an artery. He died two days later in hospital of a stroke, in what is at least the second such death in the US. Malfunctioning e-cigarette batteries have caused hundreds to thousands of similar injuries, US reports say. The Tarrant County Medical Examiner's Office found on Tuesday that shrapnel from the vape pen's exploding battery impacted Mr Brown's skull, severed his carotid artery and ultimately caused his death on 29 January. The incident took place in the parking lot of a vape shop in Fort Worth, Texas on 27 January. Mr Brown had visited the shop to seek help using a Mechanical Mod style pen - a model known to have issues, a local CBS News affiliate reported. He attempted to use the pen in the car when the battery exploded with enough force to melt plastic in the vehicle and fling metal debris into Mr Brown's face. E-cigarettes 'more harmful than we think' How likely is your e-cigarette to explode? The owners of the shop called an ambulance after seeing Mr Brown bleeding in the parking lot. "When they x-rayed him, they found the stem, the metal embedded to where the blood flows up to the brain," Mr Brown's grandmother, Alice Brown, told WFAA News. Doctors were apparently unable to remove the metal surgically. Mr Brown was placed in an induced coma, but eventually passed away. Mrs Brown, who raised Mr Brown, told the Star Telegram her grandson was just weeks away from his 25th birthday. "It just hurts so bad. Now he'll never see that birthday. It's a waste of the things he could have accomplished." The 24-year-old was a licensed electrician and not a regular smoker - he had been testing out the pen for the first time, his grandmother said. She hopes his death gives others pause before trying an e-cigarette. "If anything, I hope it stops someone," she said. "I don't know how many more people will have to die." How common is this? Last May, a 38-year-old Florida man was also killed by an exploding vape pen. Tallmadge D'Elia was burned on 80% of his body and died when metal pieces entered his skull. A US government report says there have been 195 documented cases of exploding e-cigarettes between 2009 and 2016. The National Fire Data Center found 29% of exploding vape pen incidents from January 2009 to December 2016 had caused severe injuries. Another report from the University of North Texas Health Science Center looked at US emergency room data from 2015 to 2017 and found 2,035 e-cigarette related explosion and burn injuries - far more than previous reports. The researchers said regulation and surveillance of e-cigarette devices "is urgently needed".

-
Vaping linked to increased risk for stroke, heart attack By Dennis Thompson, HealthDay News https://www.upi.com/Vaping-linked-to-increased-risk-for-stroke-heart-attack/7431548880951/ People who vape might increase their odds of suffering a stroke, heart attack or heart disease, a new study suggests. Federal survey data revealed that compared with nonusers, people who use e-cigarettes have a: 71 percent higher risk of stroke. 59 percent higher risk of heart attack or angina. 40 percent higher risk of heart disease. E-cigarette users also have a doubled rate of smoking traditional tobacco cigarettes, the researchers noted. "Even as we consider electronic cigarettes as a means of aiding in smoking cessation, we need to be careful about the impact this may have on the health of folks," said lead researcher Dr. Paul Ndunda. He is an assistant professor with the University of Kansas School of Medicine, in Wichita. The increased health risks linked to e-cigarette use held strong even after Ndunda and his colleagues accounted for other potential risk factors, such as age, excess weight, diabetes and smoking. Dr. Larry Goldstein is chairman of neurology and co-director of the Kentucky Neuroscience Institute in Lexington. He said, "This is the first real data that we're seeing associating e-cigarette use with hard cardiovascular events." Goldstein added that "it's quite a concern, especially since nationwide now we've seen a leveling off in and, in many instances, an increase in the risk of stroke-related mortality in the country. It's hard to know what contribution this has to that, but it doesn't appear to be safer, or safe right now, from the data that's available." About 3 percent of adults and 11 percent of high school students reported using e-cigarettes within the previous month in 2016, the study authors noted. In addition, vaping among young people increased by 900 percent between 2011 and 2015. For the new study, researchers gathered data on over 400,000 participants in the 2016 Behavioral Risk Factor Surveillance System, a survey regularly conducted by the U.S. Centers for Disease Control and Prevention. The researchers included nearly 66,800 people who said they had ever regularly used e-cigarettes, comparing them with about 344,000 people who'd never tried the devices. Ndunda pointed out that the nicotine in e-cigarettes probably isn't directly causing the strokes or heart health problems, since previous studies have not linked the addictive substance to plaque formation in blood vessels. "But there are other chemicals found in electronic cigarettes that could increase inflammation of the lining of the blood vessels. That could lead to clot formation, clogging the artery and causing a stroke," Ndunda said. "The vapor is not innocuous," he concluded. However, because this is survey data, it cannot draw a direct cause-and-effect relationship between vaping and stroke or heart attack, Ndunda added. "This study has some limitations that do not allow us to make very firm conclusions and be able to change policy around e-cigarettes. I would look at this as a call for larger and longer studies into this issue," Ndunda said. Goldstein, a spokesman for the American Stroke Association, agreed. "In studies of this type, it's a common problem with all of them, is that the adjustment for potential confounders is limited," Goldstein said. "They adjust it for age, sex, smoking status, diabetes and body mass index, but there are obviously other factors that can increase the risk of cardiovascular disease that weren't measured." Gregory Conley is president of the American Vaping Association, a nonprofit that advocates for sensible regulation of vaping products. He took issue with the new findings. "Nearly all regular adult users of vaping products are current smokers or ex-smokers," Conley said. "It is not exactly breaking news that [tobacco] smokers are at a far higher risk of suffering serious medical conditions, and that it takes years for some risks to subside once a smoker has quit." The study findings were to be presented Feb. 6 at the American Stroke Association's annual meeting in Honolulu. Such research is considered preliminary until published in a peer-reviewed journal. More information Harvard Medical School has more about the health effects of e-cigarettes. Copyright © 2019 HealthDay. All rights reserved.
-
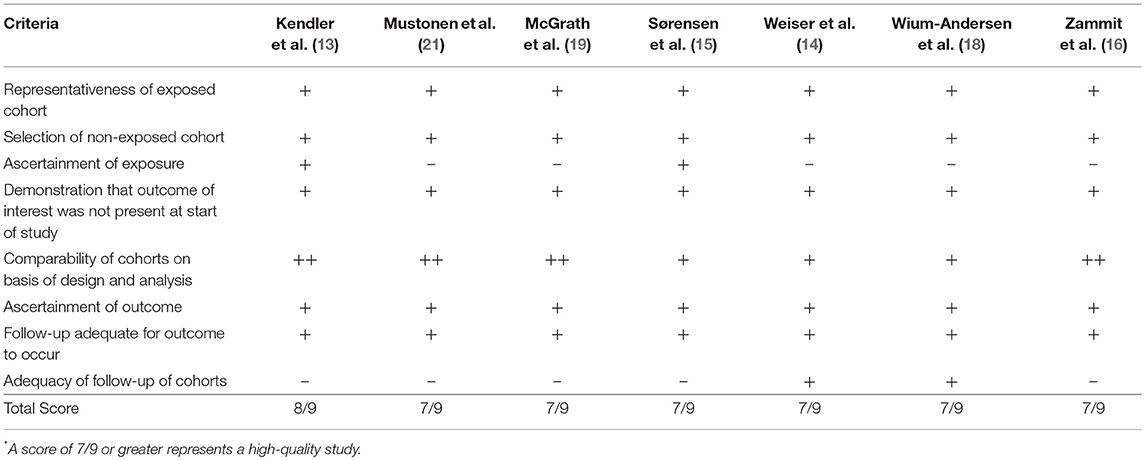
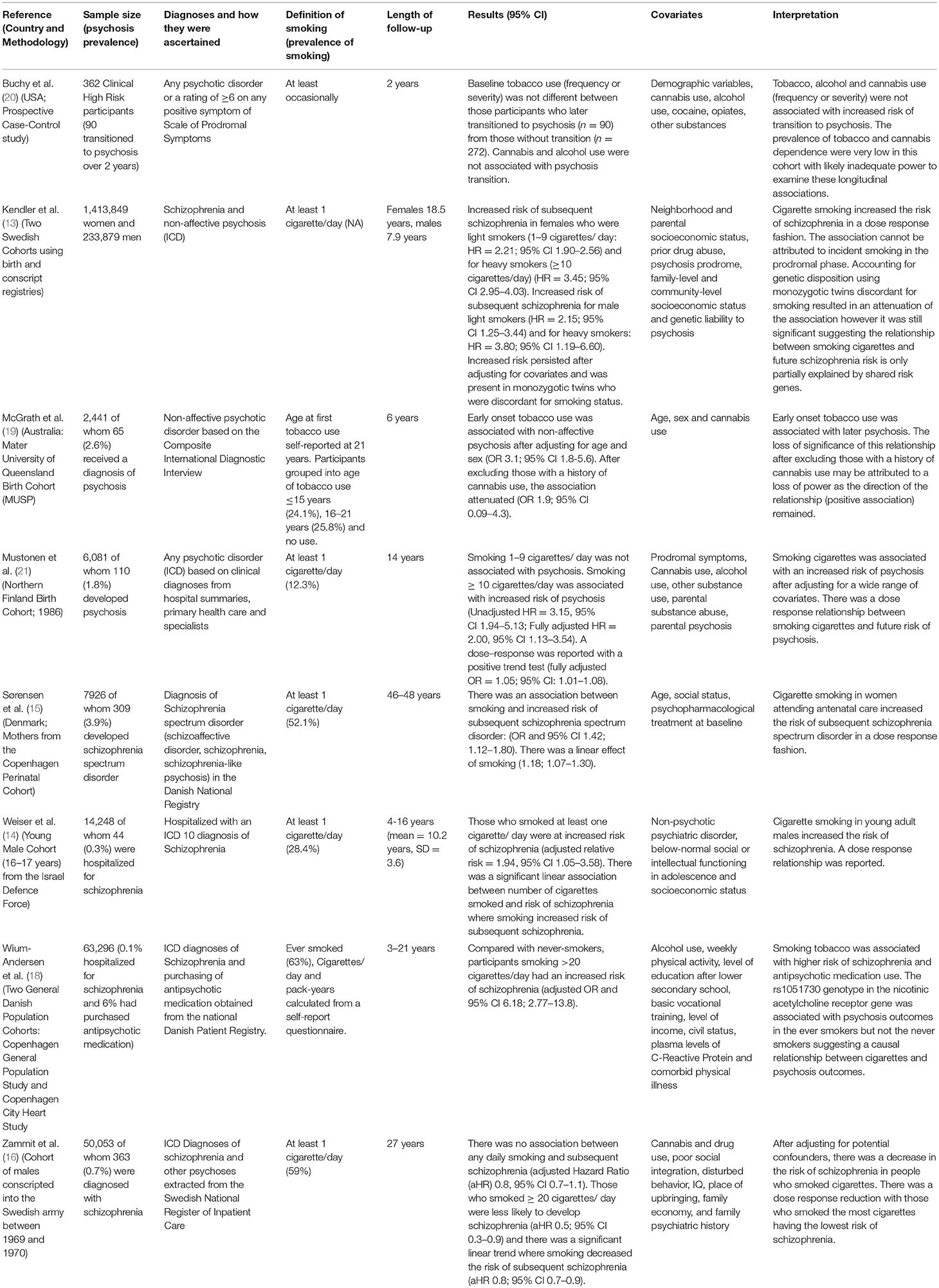
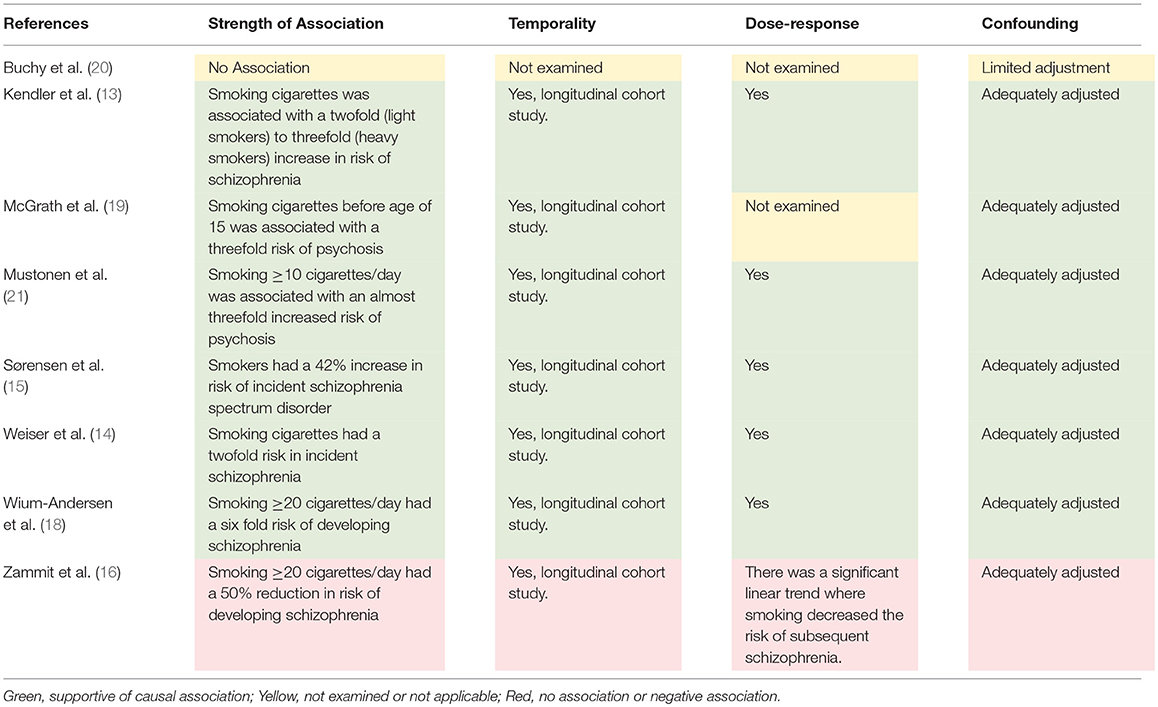
Evidence of a Causal Relationship Between Smoking Tobacco and Schizophrenia Spectrum Disorders James G. Scott, Lori Matuschka, Solja Niemelä, Jouko Miettunen, Brett Emmerson and Antti Mustonen 1Faculty of Medicine, The University of Queensland, Herston, QLD, Australia 2Queensland Centre for Mental Health Research, Wacol, QLD, Australia 3Metro North Mental Health, Royal Brisbane and Women's Hospital, Herston, QLD, Australia 4Faculty of Medicine, University of Turku, Turku, Finland 5Department of Psychiatry, South-Western Hospital District, Turku, Finland 6Center for Life Course Health Research, University of Oulu, Oulu, Finland 7Medical Research Center Oulu, Oulu University Hospital and University of Oulu, Oulu, Finland https://www.frontiersin.org/articles/10.3389/fpsyt.2018.00607/full?utm_source=AD&utm_medium=FB&utm_campaign=BLG_FPSYT_20180123 There has been emerging evidence of an association between tobacco smoking and schizophrenia spectrum disorders (SSD). Two meta-analyses have reported that people who smoke tobacco have an ~2-fold increased risk of incident schizophrenia or psychosis, even after adjusting for confounding factors. This study aimed to critically appraise the research which has examined the association between tobacco smoking and SSD against the Bradford Hill criteria for causality, to determine the strength of the evidence for a causal relationship. Eight longitudinal studies (seven cohort studies and one case control study) were identified which examined tobacco smoking as an exposure and psychosis as an outcome. All seven cohort studies were assessed as being of high quality using the Newcastle-Ottawa Scale. Six of the eight studies found a statistically significant positive association between tobacco smoking and onset of SSD. These studies reported a consistent association with a moderate to large effect size and a dose response relationship. The studies adjusted for multiple potential confounders including age, sex, socioeconomic status, shared genetic risk, prodromal symptoms, and comorbid cannabis and other substance use. The studies did not adjust for exposure to childhood trauma or prenatal tobacco. There was substantial though inconclusive evidence supporting a causal relationship between tobacco smoking and increased risk of SSD. If a causal relationship does exist, nicotine is most likely responsible for this association. This raises serious public health concerns about the increasing use of e-cigarettes and other products, particularly by adolescents whose nicotine use may increase their risk of SSD. Research is urgently needed to examine the association between e-cigarette use and incident psychosis, particularly in adolescents and young adults. Introduction Schizophrenia spectrum disorders (SSD) are heterogeneous syndromes with well-established risk factors including exposure to childhood adversity, cannabis use during adolescence, a history of obstetric complications, stressful events during adulthood, and low maternal serum folate level (1). In recent years, there has been a growing interest in tobacco smoking as a risk factor for SSD (2, 3). Tobacco smoking is known to cause a wide range of physical health problems. It is the leading cause of preventable death, through increasing the risk of lung and other malignancies, chronic obstructive pulmonary disease (COPD), coronary heart disease, cerebrovascular disease, asthma and diabetes (4). Two systematic reviews and meta-analyses have examined the association between tobacco smoking and psychotic disorders (2, 3). In pooling longitudinal studies (n = 5), Gurillo and colleagues reported a 2-fold increase in the risk of incident psychotic disorders in people who were daily tobacco smokers compared to those who were not (RR = 2.18; 95% CI 1.23–3.85). Similarly, Hunter et al. (3) who pooled data from studies identified using inclusion criteria with the outcome restricted to schizophrenia (N = 5) also reported smoking tobacco was associated with a 2-fold risk of schizophrenia (RR = 1.99; 95% CI 1.10–3.61). Both studies concluded that further research was needed to examine the potential causal role of tobacco smoking in the onset of SSD. The association between tobacco smoking and SSD is of growing significance. There is evidence that nicotine alters signaling in the dopaminergic, cholinergic, and glutamatergic neurotransmitter systems, particularly in adolescence (5). Whilst the smoking of tobacco by young people has declined in many high income countries, there has been an increase in exposure to nicotine by this demographic through the availability of e-cigarettes (6). It is therefore important to critically examine the evidence for a causal relationship between tobacco smoking and SSD. In this review we aimed to evaluate the relationship between tobacco smoking and SSD which we defined as any non-affective psychotic disorder against causal criteria based on the Bradford Hill Framework (7, 8). The Bradford Hill Framework provides nine criteria for establishing a causal relationship between an exposure and outcome. This review examined longitudinal studies identified from the two recent systematic reviews of tobacco smoking and incident SSD and other identified studies. The evidence for a causal relationship between tobacco smoking and SSD, alternative explanations for the association and the health implications are discussed. Methods Literature Search We used the results of the two recently conducted systematic reviews (2, 3) to identify studies which examined tobacco smoking as an exposure and SSD as an outcome. As the review by Hunter et al. (3) restricted the outcome to a diagnosis of schizophrenia, we used the broader search strategy of Gurillo et al. (2) to identify studies from January 2014 to May 2018 that included the broader outcome of psychosis. These psychosis outcomes included schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder, non-affective psychotic disorder, atypical psychosis, psychotic depression, and bipolar mania with psychotic features. The inclusion criteria of the current review were: (a) longitudinal case control or cohort studies; (b) study populations of participants with psychosis or schizophrenia as the outcome (defined as those who meet the diagnostic criteria by structured interview or diagnosed by treating clinician); (c) presence of tobacco smoking prior to psychosis or schizophrenia diagnosis. Studies which were cross sectional in design or only provided sub-diagnostic outcomes of psychosis (e.g., psychotic symptoms, hallucinations, delusions) were excluded. Data Extraction Titles and abstracts of the articles were reviewed to identify studies that met the eligibility criteria. The following characteristics were extracted from each study when available: (a) study methodology (including author, publication year, location, study design, follow-up period, sample numbers, loss to follow-up, age at baseline, tobacco smoking measures, and assessment of psychosis or schizophrenia), and (b) study findings (effect size metrics, 95% CI, and confounders adjusted for). The quality or the studies assessing for risk of bias was evaluated using Newcastle–Ottawa Scale (NOS) (9) as shown in Supplementary Table 1. The NOS is a method recommended by the Cochrane Non-randomized Studies Methods Working Group to evaluate the quality of the study. Points are assigned based on the selection process of cohorts (0–4 points), the comparability of the cohorts (0–2 points) and the identification of the exposures and the outcomes of research participants (0–3 points). A score of 7 or greater out of 9 was defined as high quality. Studies were assessed independently by two reviewers (LM and JS). Assessment of Causality Studies that met inclusion and exclusion criteria were assessed using causal criteria based on the Bradford Hill Framework shown in Supplementary Table 2. Of the nine criteria, five were chosen as most relevant for the purposes of this study (strength of association, consistency, temporality, dose-response, and biological plausibility). Given that smoking is known to cause a wide range of health problems, the criteria of specificity was not applicable. No studies have performed experimental manipulation exposing adolescents to tobacco because of the known harmful effects therefore this criteria was not included. Coherence was not included because of the lack of homogenous pathology evident in psychosis. In relation to analogy, the association between cannabis use and psychosis, reported to be causal (1) has some analogy to that of tobacco and psychosis. However, it is widely recognized that adolescents who smoke tobacco are more likely to smoke cannabis (10–12). Thus, cannabis rather than being analogous to tobacco in its relationship with psychosis may in fact be an important confounder. Similarly there are other important environmental factors which might confound the relationship between tobacco smoking and incident psychotic disorder. To address this concern, for the purpose of assessing evidence of causality, we included an extra criteria “accounted for confounding.” These six criteria were deemed appropriate by the research team in order to grade the associations reported between adolescent tobacco smoking and future risk of SSD as a basis for causality discussion (7). Results Gurillo and colleagues (2) identified four studies which met the specified inclusion criteria (13–16). One of the longitudinal studies (17) which they included in their pooled analysis did not determine the presence of tobacco smoking before the schizophrenia diagnosis and was therefore excluded. Hunter et al. (3) included another study (18) and the updated search identified a further three studies which met inclusion criteria (13, 19–21). In total, eight studies (seven cohort and one case-control studies) were included for assessment of a causal relationship between tobacco smoking in adolescence and incident SSD. Using the NOS, all seven cohort studies scored 7/9 or greater demonstrating they were of high quality (Table 1). Study Characteristics Table 2 summarizes the study characteristics. They utilized birth cohort studies of offspring (19, 21) or mothers (15), cohorts of young male conscripts from defense forces (14, 16), two cohorts combined, the first consisting of mothers recruited from a birth cohort, the second were male conscripts Kendler et al. (13) and two general population cohorts to assess cardiovascular risk factors (18). The longitudinal case control study was of participants at clinical high risk of psychosis (20). All studies were from high income countries. The follow-up period of all cohort studies was adequate to ascertain incident cases of SSD, ranging from a minimum of 4 years (14) to a maximum of 48 years (15). Two of the studies were genetically informed with one examining psychosis risk in family members discordant for smoking (13), the other examining schizophrenia in people with different alleles of the rs1051730 genotype in the nicotinic acetylcholine receptor gene stratified by smoking status (18). Assessment of Studies Against Bradford Hill Criteria Using causal criteria, based on the Bradford Hill Framework Hill (8), of the eight studies examined, six reported a positive association between tobacco smoking and risk of schizophrenia spectrum disorder. The strength of the associations were robust ranging from an almost 50% increased risk (15) to a 6-fold increased risk of schizophrenia in heavy smokers (18). In these six studies, all reported a temporal association with appropriate adjustment for confounding variables, particularly comorbid substance use. All but one (19) demonstrated a dose response relationship between tobacco use and SSD. By contrast, one study (16) reported that smoking tobacco reduced the risk of schizophrenia and the case control study (20) found no association. Discussion Two meta-analyses have demonstrated that smoking tobacco is associated with a 2-fold increase in risk of incident schizophrenia (3) or broader psychosis (2). Based on these systematic reviews and our own literature search, we identified eight studies that examined the longitudinal association between tobacco smoking and incident SSD of which six demonstrated a positive association (13–15, 18, 19, 21), one a negative association (16) and the final study showed no association (20). Using the Bradford Hill framework, a causal association between tobacco smoking and onset of SSD is discussed on the basis of strength of association, temporality, dose-response, adjustment for confounding factors, biological plausibility, and consistency of the association. Strength Of the six studies that found a positive association (13–15, 18, 19, 21), five reported moderate to large effect sizes (22) (Tables 2, 3) consistent with a causal relationship (8). Sørensen et al. (15) reported a smaller effect size with a 42% increase in the odds of schizophrenia spectrum disorder in people who smoked cigarettes. Consistency Consistency of the association is assessed through multiple studies of independent cohorts confirming the same result. In the eight longitudinal studies, six reported a positive association between tobacco smoking and incident SSD. Of the two which did not report a positive association, one was a case-control study of participants at clinical high risk for psychosis which found that neither tobacco nor cannabis smoking were associated with transition to psychosis. The prevalence of tobacco and cannabis dependence in this cohort was low and the study may have been underpowered to examine the effects of these substances on transition to psychosis. Zammit et al. (16) reported that smoking tobacco was associated with a lower risk of future schizophrenia, and was therefore inconsistent with the main body of research. The overwhelming majority of studies showed a positive relationship fulfilling criteria for consistency. Temporality The six studies that reported a positive association demonstrated a clear temporal relationship with the exposure of tobacco smoking preceding the onset of SSD. Schizophrenia spectrum disorders frequently have an insidious onset with a long prodrome. In order to address this concern, (21), adjusted for prodromal psychotic symptoms at baseline and Kendler et al. (13) accounted for the possible prodrome by conducting a subanalysis restricting the onset of SSD to at least 5 years following initial exposure to tobacco. The relationship between tobacco smoking and onset of schizophrenia was largely attenuated after accounting for the prodrome rendering reverse causality an unlikely explanation for the association between tobacco use and SSD thus suggesting tobacco smoking precedes the illness. Dose-Response A dose response between tobacco smoking and incident SSD was reported in five of the six studies reporting a positive association. In three studies (14, 15, 21) a significant linear trend was demonstrated where the risk of SSD increased with the an increase in tobacco smoking. In two studies (13, 18), those who smoked more daily tobacco had an increase in the odds of developing SSD. Potential Confounders The relationship between tobacco use and SSD remained significant even after adjusting for factors that might confound the relationship including family socio-economic status, cannabis use (1), parental substance abuse and parental psychosis (23–27). A shared genetic liability was also accounted for in two genetically informed studies (13, 18). Adjustment for confounders attenuated the strength of the association but significance was maintained in all but one study (19), probably due to a lack of power for the analysis. None of the studies adjusted for childhood trauma (28). Biological Plausibility Tobacco and tobacco smoke contain almost 5,000 different chemicals. Nicotine is the most important pharmacologically active and psychotogenic compound in tobacco smoke because of its interaction with nicotinic acetylcholine receptors (29). Previous reports on tobacco smoking suggests that nicotine could alter signaling of dopaminergic, cholinergic, and glutamatergic neurotransmitter systems (5, 30) and thus could potentially influence brain development as suggested by studies of adolescent nicotine exposure and neurodevelopmental trajectories (5). Also, excess nicotine intake during early adolescence is associated with abnormal white matter maturation in adults (31), and chronic cigarette smoking has been linked to structural brain changes such as gray matter decreases in the prefrontal cortex, which correspond with areas where functional alterations occur from nicotine exposure (32). Furthermore, recent evidence suggest that adolescent nicotine use could have persistent effects on nicotine receptor responsiveness, which results in the strengthening of negative emotional changes and alterations in cognitive functioning (5). Alternative Explanations There are other explanations for the positive association between tobacco smoking and SSD. Individuals who develop schizophrenia are more likely to have externalizing symptoms in childhood and adolescence (33, 34) and children with externalizing symptoms are more likely to smoke tobacco during adolescence (35). There may be unmeasured confounding. None of the studies adjusted for childhood trauma, a well-established risk factor for SSD (1, 28) and for tobacco use (36). Similarly there was no adjustment for prenatal tobacco smoking exposure which is associated with both an increased risk of smoking in adolescence (37) and an increased risk of schizophrenia even after adjusting for life time smoking (3, 38). Furthermore, recent studies have suggested bidirectional associations by revealing single nucleotide polymorphisms associated with nicotine dependence (CHRNA5) that are also associated with schizophrenia (39, 40). Limitations Each study included in this review is observational in methodology, and the majority of cohort studies included had significant attrition. Participants who are most likely to be lost to follow up are more likely to be socioeconomically disadvantaged and be at increased risk of both tobacco smoking and mental illness. Therefore, it is unlikely that attrition would significantly affect reported associations. Measurement of tobacco smoking has been measured via self-report or by interview, generally at one point in time and often retrospectively recalled. Only one study measured the long-term smoking exposure prior the psychotic illness using pack-years (18) which provides a more precise measurement of tobacco smoke exposure. Further, no studies have used biological markers for tobacco smoking such as expired air carbon monoxide (41) or serum cotinine measurement (42). These limitations are inherent to large cohort and registry studies and are difficult to overcome. Finally, as two recent systematic reviews had been published on this topic, we relied on these to identify the studies included in this review rather than replicating the searches in these studies. Implications Given tobacco is known to have widespread adverse health outcomes and governments around the world are adopting policies to reduce tobacco smoking, why is it important to clarify if smoking tobacco has a causal role in the onset of SSD? The first reason is that better understanding the aetiopathogenesis of SSD will inform our knowledge of this syndrome which may lead to better treatments. The second, a much more urgent consideration is the growing availability of electronic (e) cigarettes. These have been developed as a safer alternative to cigarettes by enabling nicotine use without the exposure to carcinogenic chemicals associated with smoking tobacco. However, there is growing use of e-cigarettes and other nicotine products by adolescents (6) and it is acknowledged that the health effects of e-cigarettes on youth are not fully understood (43). In addition to tobacco and cannabis, there is now evidence that adolescents who use inhalants are at increased risk of psychotic disorders (44) suggesting that adolescence is the developmental period where adverse neuropsychiatric outcomes from psychoactive substances are most likely to occur. There is substantial though not conclusive evidence that the association between tobacco smoking and SSD is causal and may well be a result of the effects of nicotine on multiple neurotransmitter systems. Therefore, policy makers must be cautious when developing regulations for the availability of e-cigarettes, nicotine replacement therapy products and smokeless tobacco. Similarly, health practitioners who recommend e-cigarettes or smokeless tobacco products as a safe alternative to smoking need to consider the findings of the studies identified in this review, especially when providing advice to adolescents. It is essential that future well designed observational studies are undertaken examining the risk of SSDs in those who use e-cigarettes, particularly in adolescence. A major challenge is the low prevalence of SSD. Recruiting samples large enough to examine the association between e-cigarettes and SSD will take many years. Previous longitudinal research has shown positive associations between cannabis, tobacco and alcohol use and psychotic experiences (PE) which are proxy markers for psychosis risk. PE have the advantage of being higher in prevalence compared to SSD thereby reducing the required sample size to identify associations. Schizophrenia endophenotypes may also have a role to inform the association between nicotine exposure through e-cigarettes and risk of SSD. Previous research has shown that smoking tobacco modulates the association between polymorphisms of transcription factor 4 and reduced sensory gating, an endophenotype of schizophrenia suggesting that the smoking of tobacco might play a role in early information processing deficits in schizophrenia (45). Use of research paradigms such as PE and endophenotypes PE would expedite research into the association between e-cigarette use and SSD risk. Further research is urgently needed to determine if nicotine is causally associated with incident SSD. In the interim, it is important that policy makers consider the available evidence between tobacco smoking and risk of schizophrenia when evaluating the potential health consequences that might arise from community access to e-cigarettes. Author Contributions JS and AM planned the review. LM conducted the initial literature search and JS and LM assessed papers for suitability for inclusion. JS and LM reviewed all the papers and assessed them for quality. JS, LM, and AM wrote the first draft of the manuscript and all authors contributed to further drafts. All authors reviewed and approved the final draft. Funding JS is supported by a National Health and Medical Research Council Practitioner Fellowship Grant APP1105807 and employed by The Queensland Centre for Mental Health Research which receives core funding from the Queensland Health. AM is supported by Juho Vainio Foundation, Scholarship Fund of the University of Oulu, Oulun Lääketieteellinen tutkimussäätiö and The Hospital District of South Ostrobothnia, Finland. JM is supported by Academy of Finland (#268336). Conflict of Interest Statement The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Supplementary Material The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2018.00607/full#supplementary-material References 1. Belbasis L, Köhler CA, Stefanis N, Stubbs B, Os Jv, Vieta E, et al. Risk factors and peripheral biomarkers for schizophrenia spectrum disorders: an umbrella review of meta-analyses. Acta Psychiatr Scand. (2018) 137:88–97. doi: 10.1111/acps.12847 PubMed Abstract | CrossRef Full Text | Google Scholar 2. Gurillo P, Jauhar S, Murray RM, MacCabe JH. Does tobacco use cause psychosis? Systematic review and meta-analysis. Lancet Psychiatry (2015) 2:718–25. doi: 10.1016/S2215-0366(15)00152-2 PubMed Abstract | CrossRef Full Text | Google Scholar 3. Hunter A, Murray R, Asher L, Leonardi-Bee J. The effects of tobacco smoking, and prenatal tobacco smoke exposure, on risk of schizophrenia: a systematic review and meta-analysis. Nicotine Tob Res. (2018). doi: 10.1093/ntr/nty160. [Epub ahead of print]. PubMed Abstract | CrossRef Full Text | Google Scholar 4. Collaborators GT. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet (2017) 389:1885–906. doi: 10.1016/s0140-6736(17)30819-x CrossRef Full Text | Google Scholar 5. Smith RF, McDonald CG, Bergstrom HC, Ehlinger DG, Brielmaier JM. Adolescent nicotine induces persisting changes in development of neural connectivity. Neurosci Biobehav Rev (2015) 55:432–43. doi: 10.1016/j.neubiorev.2015.05.019 PubMed Abstract | CrossRef Full Text | Google Scholar 6. Perikleous EP, Steiropoulos P, Paraskakis E, Constantinidis TC, Nena E. E-cigarette use among adolescents: an overview of the literature and future perspectives. Front Public Health (2018) 6:86. doi: 10.3389/fpubh.2018.00086 PubMed Abstract | CrossRef Full Text | Google Scholar 7. Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the bradford hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol. (2015) 12:14. doi: 10.1186/s12982-015-0037-4 PubMed Abstract | CrossRef Full Text | Google Scholar 8. Hill AB. The environment and disease: association or causation? Proc R Soc Med. (1965) 58:295–300. Google Scholar 9. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa: The Ottawa Hospital (2018). Google Scholar 10. Hindocha C, Shaban NDC, Freeman TP, Das RK, Gale G, Schafer G, et al. Associations between cigarette smoking and cannabis dependence: a longitudinal study of young cannabis users in the United Kingdom. Drug Alcohol Depend. (2015) 148:165–71. doi: 10.1016/j.drugalcdep.2015.01.004 PubMed Abstract | CrossRef Full Text | Google Scholar 11. Badiani A, Boden JM, De Pirro S, Fergusson DM, Horwood LJ, Harold GT. Tobacco smoking and cannabis use in a longitudinal birth cohort: evidence of reciprocal causal relationships. Drug Alcohol Depend. (2015) 150:69–76. doi: 10.1016/j.drugalcdep.2015.02.015 PubMed Abstract | CrossRef Full Text | Google Scholar 12. Weinberger AH, Platt J, Copeland J, Goodwin RD. Is cannabis use associated with increased risk of cigarette smoking initiation, persistence, and relapse? longitudinal data from a representative sample of US adults. J Clin Psychiatry (2018) 79:17m11522. doi: 10.4088/JCP.17m11522 PubMed Abstract | CrossRef Full Text | Google Scholar 13. Kendler KS, Lönn SL, Sundquist J, Sundquist K. Smoking and schizophrenia in population cohorts of swedish women and men: a prospective co-relative control study. Am J Psychiatry (2015) 172:1092–100. doi: 10.1176/appi.ajp.2015.15010126 PubMed Abstract | CrossRef Full Text | Google Scholar 14. Weiser M, Reichenberg A, Grotto I, Yasvitzky R, Rabinowitz J, Lubin G, et al. Higher rates of cigarette smoking in male adolescents before the onset of schizophrenia: a historical-prospective cohort study. Am J Psychiatry (2004) 161:1219–23. doi: 10.1176/appi.ajp.161.7.1219 PubMed Abstract | CrossRef Full Text | Google Scholar 15. Sørensen HJ, Mortensen EL, Reinisch JM, Mednick SA. A prospective study of smoking in young women and risk of later psychiatric hospitalization. Nordic J Psychiatry (2011) 65:3–8. doi: 10.3109/08039481003786386 PubMed Abstract | CrossRef Full Text | Google Scholar 16. Zammit S, Allebeck P, Dalman C, Lundberg I, Hemmingsson T, Lewis G. Investigating the association between cigarette smoking and schizophrenia in a cohort study. Am J Psychiatry (2003) 160:2216–21. doi: 10.1176/appi.ajp.160.12.2216 PubMed Abstract | CrossRef Full Text | Google Scholar 17. Riala K, Hakko H, Isohanni M, Pouta A, Räsänen P. Is initiation of smoking associated with the prodromal phase of schizophrenia? J Psychiatry Neurosci. (2005) 30:26–32. PubMed Abstract | Google Scholar 18. Wium-Andersen MK, Orsted DD, Nordestgaard BG. Tobacco smoking is causally associated with antipsychotic medication use and schizophrenia, but not with antidepressant medication use or depression. Int J Epidemiol. (2015) 44:566–77. doi: 10.1093/ije/dyv090 CrossRef Full Text | Google Scholar 19. McGrath JJ, Alati R, Clavarino A, Williams GM, Bor W, Najman JM, et al. Age at first tobacco use and risk of subsequent psychosis-related outcomes: a birth cohort study. Aust N Z J Psychiatry (2016) 50:577–83. doi: 10.1177/0004867415587341 PubMed Abstract | CrossRef Full Text | Google Scholar 20. Buchy L, Cadenhead KS, Cannon TD, Cornblatt BA, McGlashan TH, Perkins DO, et al. Substance use in individuals at clinical high risk of psychosis. Psychol Med. (2015) 45:2275–84. doi: 10.1017/S0033291715000227 PubMed Abstract | CrossRef Full Text | Google Scholar 21. Mustonen A, Ahokas T, Nordström T, Murray GK, Mäki P, Jääskeläinen E, et al. Smokin‘ hot: adolescent smoking and the risk of psychosis. Acta Psychiatr Scand. (2018) 138:5–14. doi: 10.1111/acps.12863 PubMed Abstract | CrossRef Full Text | Google Scholar 22. Rosenthal JA. Qualitative descriptors of strength of association and effect size. J Soc Serv Res. (1996) 21:37–59. doi: 10.1300/J079v21n04_02 CrossRef Full Text | Google Scholar 23. McAdams TA, Neiderhiser JM, Rijsdijk FV, Narusyte J, Lichtenstein P, Eley TC. Accounting for genetic and environmental confounds in associations between parent and child characteristics: a systematic review of children-of-twins studies. Psychol Bull. (2014) 140:1138–73. doi: 10.1037/a0036416 PubMed Abstract | CrossRef Full Text | Google Scholar 24. Niemi-Pynttäri JA, Sund R, Putkonen H, Vorma H, Wahlbeck K, Pirkola SP. Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases. J Clin Psychiatry (2013) 74:e94–9. doi: 10.4088/JCP.12m07822 PubMed Abstract | CrossRef Full Text | Google Scholar 25. Patrick ME, Wightman P, Schoeni RF, Schulenberg JE. Socioeconomic status and substance use among young adults: a comparison across constructs and drugs. J Stud Alcohol Drugs (2012) 73:772–82. doi: 10.15288/jsad.2012.73.772 PubMed Abstract | CrossRef Full Text | Google Scholar 26. Radhakrishnan R, Wilkinson ST, D'Souza DC. Gone to pot - a review of the association between cannabis and psychosis. Front Psychiatry (2014) 5:54. doi: 10.3389/fpsyt.2014.00054 PubMed Abstract | CrossRef Full Text | Google Scholar 27. Starzer MSK, Nordentoft M, Hjorthøj C. Rates and predictors of conversion to schizophrenia or bipolar disorder following substance-induced psychosis. Am J Psychiatry (2018) 175:343–50. doi: 10.1176/appi.ajp.2017.17020223 PubMed Abstract | CrossRef Full Text | Google Scholar 28. Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, Viechtbauer W, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. (2012) 38:661–71. doi: 10.1093/schbul/sbs050 PubMed Abstract | CrossRef Full Text | Google Scholar 29. Thielen A, Klus H, Müller L. Tobacco smoke: unraveling a controversial subject. Exp Toxicol Pathol. (2008) 60:141–56. doi: 10.1016/j.etp.2008.01.014 PubMed Abstract | CrossRef Full Text | Google Scholar 30. Davis J, Eyre H, Jacka FN, Dodd S, Dean O, McEwen S, et al. A review of vulnerability and risks for schizophrenia: Beyond the two hit hypothesis. Neurosci Biobehav Rev. (2016) 65:185–94. doi: 10.1016/j.neubiorev.2016.03.017 PubMed Abstract | CrossRef Full Text | Google Scholar 31. Gogliettino AR, Potenza MN, Yip SW. White matter development and tobacco smoking in young adults: a systematic review with recommendations for future research. Drug Alcohol Depend. (2016) 162:26–33. doi: 10.1016/j.drugalcdep.2016.02.015 PubMed Abstract | CrossRef Full Text | Google Scholar 32. Sutherland MT, Riedel MC, Flannery JS, Yanes JA, Fox PT, Stein EA, et al. Chronic cigarette smoking is linked with structural alterations in brain regions showing acute nicotinic drug-induced functional modulations. Behav Brain Funct. (2016) 12:16. doi: 10.1186/s12993-016-0100-5 PubMed Abstract | CrossRef Full Text | Google Scholar 33. Scott J, Martin G, Welham J, Bor W, Najman J, O'Callaghan M, et al. Psychopathology during childhood and adolescence predicts delusional-like experiences in adults: a 21-year birth cohort study. Am J Psychiatry (2009) 166:567–74. doi: 10.1176/appi.ajp.2008.08081182 PubMed Abstract | CrossRef Full Text | Google Scholar 34. Matheson SL, Shepherd AM, Laurens KR, Carr VJ. A systematic meta-review grading the evidence for non-genetic risk factors and putative antecedents of schizophrenia. Schizophr Rese. (2011) 133:133–42. doi: 10.1016/j.schres.2011.09.020 PubMed Abstract | CrossRef Full Text | Google Scholar 35. Miettunen J, Murray GK, Jones PB, Maki P, Ebeling H, Taanila A, et al. Longitudinal associations between childhood and adulthood externalizing and internalizing psychopathology and adolescent substance use. Psychol Med. (2014) 44:1727–38. doi: 10.1017/S0033291713002328 PubMed Abstract | CrossRef Full Text | Google Scholar 36. Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. (2012) 9:e1001349. doi: 10.1371/journal.pmed.1001349 PubMed Abstract | CrossRef Full Text | Google Scholar 37. Niemela S, Raisanen A, Koskela J, Taanila A, Miettunen J, Ramsay H, et al. The effect of prenatal smoking exposure on daily smoking among teenage offspring. Addiction (2017) 112:134–43. doi: 10.1111/add.13533 PubMed Abstract | CrossRef Full Text | Google Scholar 38. Niemela S, Sourander A, Surcel HM, Hinkka-Yli-Salomaki S, McKeague IW, Cheslack-Postava K, et al. Prenatal nicotine exposure and risk of schizophrenia among offspring in a national birth cohort. Am J Psychiatry (2016) 173:799–806. doi: 10.1176/appi.ajp.2016.15060800 PubMed Abstract | CrossRef Full Text | Google Scholar 39. Chen J, Bacanu SA, Yu H, Zhao Z, Jia P, Kendler KS, et al. Genetic relationship between schizophrenia and nicotine dependence. Sci Rep. (2016). 6:25671. doi: 10.1038/srep25671. PubMed Abstract | CrossRef Full Text | Google Scholar 40. Hartz SM, Horton AC, Hancock DB, Baker TB, Caporaso NE, Chen LS, et al. Genetic correlation between smoking behaviors and schizophrenia. Schizophr Res. (2018) 194:86–90. doi: 10.1016/j.schres.2017.02.022 PubMed Abstract | CrossRef Full Text | Google Scholar 41. Jarvis MJ, Russell MA, Saloojee Y. Expired air carbon monoxide: a simple breath test of tobacco smoke intake. Br Med J. (1980) 281:484–5. PubMed Abstract | Google Scholar 42. Vartiainen E, Seppala T, Lillsunde P, Puska P. Validation of self reported smoking by serum cotinine measurement in a community-based study. J Epidemiol Commun Health (2002) 56:167–70. doi: 10.1136/jech.56.3.167 PubMed Abstract | CrossRef Full Text | Google Scholar 43. National Academies of Sciences Engineering and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems. Public Health Consequences of E-Cigarettes. In: Eaton DL, Kwan LY, Stratton K, editors. Washington, DC: National Academies Press (US) (2018). 44. Mustonen A, Niemela S, McGrath JJ, Murray GK, Nordstrom T, Maki P, et al. Adolescent inhalant use and psychosis risk-a prospective longitudinal study. Schizophr Res. (2018). doi: 10.1016/j.schres.2018.05.013. [Epub ahead of print]. PubMed Abstract | CrossRef Full Text | Google Scholar 45. Quednow BB, Brinkmeyer J, Mobascher A, Nothnagel M, Musso F, Grunder G, et al. Schizophrenia risk polymorphisms in the TCF4 gene interact with smoking in the modulation of auditory sensory gating. Proc Natl Acad Sci USA. (2012) 109:6271–6. doi: 10.1073/pnas.1118051109 PubMed Abstract | CrossRef Full Text | Google Scholar
-
Rant
MarylandQuitter replied to Christa326's topic in Discussion: Vaping & Juuling - Another Generation At Risk
I think everybody is looking at the same forest but the trees are getting in the way. The bottom line is, whether NRT is used or not, the goal is to get off of nicotine completely and for good. The use of NRT delays nicotine withdrawal but again, that's okay so long as the goal is to stop nicotine for good, and much sooner than later. There is no one right way to quit but there is only one way to stay quit and that is to NEVER TAKE ANOTHER PUFF, EVER. I used Wellbutrin to quit and it worked for me. No need for anybody to look in the past because as long as we're not smoking and not using nicotine in any form, we've succeeded at stomping nicotine addiction out of lives and much, much less of a chance of relapse. Our philosophy on quitting smoking: Quit Train®, a quit smoking support community, was created by former smokers who have a deep desire to help people quit smoking and to help keep those quits intact. This place should be a safe haven to escape the daily grind and focus on protecting our quits. We don't believe that there is a "one size fits all" approach when it comes to quitting smoking. Each of us has our own unique set of circumstances which contributes to how we go about quitting and more importantly, how we keep our quits. This is not an environment where anybody will be judged as we only exist to offer education, support and acceptance. Through education and sharing experiences, we can all help each other to keep this nasty, deadly addiction out of our lives. We all want the same thing; to stay smoke-free and enjoy our lives of living as a non-smoker and all of the health benefits and freedom that it offers. Anybody can quit smoking and anybody can stay that way. It's a matter of finding a good combination of education and support to expose the lies of smoking in a comfortable, come as you are environment. We welcome all with open arms and hope that you can make this your safe haven to take your freedom back and get on with the business of living life as a non-smoker. -
notsmokinjo, That's awesome! You had a conversation with those children that they probably won't ever forget. It's fantastic that you had the opportunity to talk to your daughter and a group of her friends about smoking and vaping. That's really paying it forward. Very cool that they were able to use QT for a research tool. I love it! Oh, you might have already seen article about nicotine found in vape liquids, despite it being illegal in AT, but in case you haven't...
-
mpower download from WHO mpower_english.pdf
-
- 1
-

-
I have a 9 year old daughter who remembers when I used to smoke. This is a conversation that has come up from time-to-time since I quit but even more so now, because I bring up smoking and vaping to her, which leads to a lot of questions from her. The superintendent of her school system sent an email to all of the parents about the kids vaping. I talked to her about this and explained to her about the nasty things that come along with vaping. Things like heavy metals, how the heavy metals get into the vapor and how dangerous it actually is and of course the dangers of nicotine addiction. I want her to not even be tempted to try any of this but if she ever is, I want her to know the truth behind all of the clever marketing targeting our children. This is 1970's tobacco advertising all over again. As former smokers who are educated about addiction and how to beat it, there is nobody more qualified to reach kids and stop this epidemic from going any further. Moreover, there also is nobody better than us to talk to kids who are already vaping (or smoking) and addicted and help them to quit. We're experts in this field and talk about paying it forward, this is our chance. Do any members here have school age children, nieces, nephews, grandchildren etc. and if so, have you talked to them about this? There are lots if educational articles and videos about the dangers of vaping and juuling on the new board: Vaping & Juuling: Unquestionable Addiction, Reckless Aftermath The concerted efforts of big tobacco corporations - same drug, new package, new demographic; our youth.
-
For anyone thinking of having a ciggerette
MarylandQuitter replied to Whispers's topic in Quit Smoking Discussions
My 9 year old daughter asked me the other day if my lungs were more black or pink. I talk to her about smoking, vaping etc. so she knows the truth about this stuff. My Mom and my Aunt have never taken a single puff of a cigarette, despite growing up with both parents who smoked, all her brothers, uncles, aunts etc. My goal is to teach my daughter now so she knows the consequences of smoking, vaping etc. so she doesn't even want to try any of it. -
Rant
MarylandQuitter replied to Christa326's topic in Discussion: Vaping & Juuling - Another Generation At Risk
Some members here are still smoking, trying to quit. That's okay. This is where they need to be. Some are using NRT products. However, that is fine so long as the NRT is short-term, very short-term because the goal is to get off of nicotine completely. The sooner the better which is why the cold turkey method have the most success. It's not the only method that works, but it is the method of quitting that has best success rates, hands down. Anybody who is vaping any amount of nicotine is not quit. This is not even worth debating because the person is still putting nicotine into their body and keeping the drug addiction alive and well; they're only lying to themselves, as all using drug addicts do. See this board for everything you need to know about vaping. Vaping & Juuling: Unquestionable Addiction, Reckless Aftermath -
Two Weeks, 14 Days, and On to week #3
MarylandQuitter replied to Opah's topic in Quit Smoking Discussions
Congratulations! Glad to see you're celebrating! You deserve it because staying quit for two weeks is no small feat! ? -
NOPE!
-
https://www.tobaccofreekids.org/what-we-do/industry-watch/e-cigarettes Introduced in 2015, Juul electronic cigarettes have quickly skyrocketed in popularity among teens and college students across the United States, according to widespread news reports. Educators and students report an alarming level of Juul use in middle and high schools, making this an urgent public health problem. Several factors have contributed to Juul’s rising popularity with teens: Juul e-cigarettes are sleek, high tech and easy to hide. They look just like USB flash drives and can be charged in the USB port of a computer. They don’t look anything like a traditional tobacco product. A Juul is also small enough to fit in a closed hand. Juul comes in sweet flavors that appeal to youth, including mango, fruit medley, crème brulee, cool mint and cool cucumber. Research has shown that flavors play a key role in youth use of tobacco products, including e-cigarettes. Juul appears to deliver nicotine more quickly, more effectively and at higher doses than other e-cigarettes, increasing users’ risk of addiction. The manufacturer claims each Juul cartridge of nicotine liquid (called a “Juul pod”) contains as much nicotine as a pack of cigarettes (about 200 puffs). However, research has found that many Juul users don’t know the product always contains nicotine, and many teens call use of the product “juuling,” indicating they may not realize it is an e-cigarette or tobacco product. Juul sales have grown dramatically and now make up more than half the e-cigarette market. Juul is putting kids at risk of nicotine addiction and threatens to undermine decades of progress in reducing youth tobacco use: A 2016 Surgeon General’s report concluded that youth use of nicotine in any form, including e-cigarettes, is unsafe, can cause addiction and can harm the developing adolescent brain. A January 2018 report by the National Academies of Sciences, Engineering and Medicine concluded, “There is substantial evidence that e-cigarette use increases risk of ever using combustible tobacco cigarettes among youth and young adults.” The alarming increase in youth use of Juul requires strong and immediate action by the Food and Drug Administration to protect kids. The FDA is responsible for regulating tobacco products, including e-cigarettes, and the FDA must take action to address the skyrocketing youth use of Juul.
-
FYI, Altria owns Philip Morris Statement of Matthew L. Myers, President, Campaign for Tobacco-Free Kids December 20, 2018 https://www.tobaccofreekids.org/press-releases/2018_12_20_altria_juul WASHINGTON, D.C. – The announcement that Altria is buying a 35 percent stake in Juul is a truly alarming development for public health and brings together the two companies that have been the most successful in marketing their highly addictive products to kids. Public health is the loser in a deal that joins America’s most powerful cigarette company, whose success has been driven by Marlboro’s appeal to our youth, and the company responsible for the explosive growth in e-cigarette use among our nation’s children. Altria has no interest in reducing the number of people who smoke cigarettes. They see Juul as their failsafe in case the cigarette market keeps declining so that they remain profitable no matter what happens. Altria’s interests are served by maximizing sales and profits from both the cigarette and e-cigarette markets, and they have every reason to push Juul to market its products in a way that does the least damage to the cigarette market. As for Juul, the company has lost all credibility in claiming that it cares about public health. There is no longer any question that Juul has been the driving force behind the skyrocketing youth e-cigarette epidemic that has teens and families across the country struggling to deal with nicotine addiction. Juul’s growth has been powered by its success in addicting kids, and the company’s owners have just become billionaires as a result. This deal also creates a political behemoth that is likely to increase the already huge sums these companies spend to fight regulatory and legislative efforts to discourage use of their products. This deal underscores the urgent need for effective FDA regulation of e-cigarettes and all tobacco products to stop tobacco companies from reversing decades of progress and addicting another generation of kids. The FDA should strengthen its efforts to address the youth e-cigarette epidemic by prohibiting all flavored e-cigarettes that have not been subject to public health review by the agency, stopping online sales of e-cigarettes until stronger safeguards are in place to prevent sales to kids, restricting marketing that appeals to kids, and enforcing rules prohibiting the sale of new products without prior FDA review and authorization. It is also critical that the FDA quickly implement its proposals to accelerate reductions in use of cigarettes and other combustible tobacco products. These include banning menthol cigarettes and flavored cigars and reducing nicotine levels in cigarettes to non-addictive or minimally addictive levels (and it should extend the latter proposal to other combustible products). The Altria-Juul deal shows how far the tobacco industry will go to maximize profits and sell as many products as possible, including cigarettes. The FDA and other policymakers must be equally aggressive in working to reduce tobacco use and save lives.
-
Video discusses how former smokers have first hand knowledge of how they got trapped into nicotine addiction and how they can use that experience to their advantage to help prevent young people they care about from making the same mistake.
-
Video discusses how nicotine addiction takes a toll on all users, even if they are lucky enough to never go on to develop any major medical problems associated with its use.
-
- 1
-

-
NOPE!
-
A study at the University of Birmingham shows the effect of vaping liquid after being inhaled, and it's not good. Derek Beres 21 August, 2018 Here we go again. Advocates for a “healthier” alternative to cigarettes took another hit from a recent study published in the journal, Thorax. A number of previous studies have focused on e-cigarette liquid before being vaped. For this research, University of Birmingham coauthor Dr. David Thickett, a professor in the Institute of Inflammation and Ageing, investigated the effects on the lungs after inhalation. Thickett and his team took tissue samples from eight nonsmokers to study the effects of the liquid over the next 48 hours. They discovered that the vapor causes the production of inflammatory cytokines, as well as the inhibition of a cellular “safety device,” phagocytosis. Simply put: "We show a significant increase in cytotoxicity caused by the vaping process itself." Cytokines are a broad group of proteins that affect local cells. They are particularly critical in the functioning of the immune system. They help determine the body’s response to a host of potential issues, including cancer, sepsis, trauma, and, as this study shows, inflammation. Vaping increases inflammatory behavior in lung tissue cells. It also decreases the efficacy of a process called phagocytosis, in which pathogens and cell debris are removed from the immune system. As the inflammatory cell response is increasing, the very mechanism that helps combat it is silenced. The popularity of vaping continues, however. In 2017, over one-quarter of high school seniors and 13 percent of eighth graders claimed they vaped. Research shows that college freshmen who vape are more likely to indulge in cigarettes as well. But when a company like Juul is valued at $16 billion, chances that we'll slow down are slim. And so the debate regarding the safety of cigarettes versus e-cigs continues. Thickett notes that there are still fewer carcinogens in the vaping liquid. In this sense, vaping appears safer than cigarettes. Yet Thickett says that in 20 or 30 years time, chronic obstructive pulmonary disease remains a real possibility for e-cig users. "I don’t believe e-cigarettes are more harmful than ordinary cigarettes. But we should have a cautious scepticism that they are as safe as we are being led to believe." The authors of the study also note that they have not studied the flavors used in vaping liquid, which could promote further toxic effects. The lesson remains: nothing goes into your lungs without consequence. The question is how much of a risk you’re willing to take.
-
- 4
-
-
-
https://www.lung.org/stop-smoking/smoking-facts/e-cigarettes-and-lung-health.html E-Cigarettes Electronic cigarettes, or e-cigarettes, are tobacco products that have been sold in the U.S. for about a decade. They include e-pens, e-pipes, e-hookah, and e-cigars, known collectively as ENDS—electronic nicotine delivery systems. They’re also sometimes called JUULs, "vapes" and "vape pens." E-cigarettes are the most commonly used tobacco products among kids—and it’s become an epidemic. While much remains to be determined about the lasting health consequences of e-cigarettes, there’s evolving evidence about the health risks of e-cigarettes on the lungs—including irreversible lung damage and lung disease. The American Lung Association is very concerned that we are at risk of losing another generation to tobacco-caused diseases as the result of e-cigarettes. The Lung Association remains extremely troubled about the rapid increase of youth using these products and has repeatedly called upon the Food and Drug Administration (FDA) to increase their oversight and scrutiny of these products to protect kids. What You Need to Know About E-Cigarettes Below are answers to common questions about e-cigarettes, including health consequences, risks of secondhand emissions, kids and e-cigarettes and FDA oversight. What Are E-Cigarettes? Electronic cigarettes, or e-cigarettes, include e-pens, e-pipes, e-hookah, and e-cigars are known collectively as ENDS— electronic nicotine delivery systems. According to the FDA, e-cigarettes are devices that allow users to inhale an aerosol containing nicotine or other substances. Unlike traditional cigarettes, e-cigarettes are generally battery-operated and use a heating element to heat e-liquid from a refillable cartridge, releasing a chemical-filled aerosol. What's in E-Cigarettes? The main component of e-cigarettes is the e-liquid contained in cartridges. To create an e-liquid, nicotine is extracted from tobacco and mixed with a base (usually propylene glycol), and may also include flavorings, colorings and other chemicals (such as formaldehyde and acrolein, which can cause irreversible lung damage). Are E-Cigarettes a Gateway to Youth Smoking? The National Academies of Science, Engineering and Medicine concluded there is "substantial evidence" that if a youth or young adult uses an e-cigarette, they are at increased risk of using traditional cigarettes. What Are the Health Consequences of E-Cigarette Use? A recent study from the University of North Carolina found that even in small doses, inhaling the two primary ingredients found in e-cigarettes—propylene glycol and vegetable glycerin—is likely to expose users to a high level of toxins and that the more ingredients a user is inhaling, the greater the toxicity.1 The mid-to-long-term consequences of e-cigarettes are not yet known, as it's a new product and has been sold for less than a decade in the U.S. While much remains to be determined about these lasting health consequences of these products, we are very troubled by what we see so far. The inhalation of harmful chemicals can cause irreversible lung damage and lung diseases. Can E-Cigarettes Help Smokers Quit? The Food and Drug Administration has not found any e-cigarette to be safe and effective in helping smokers quit. If smokers are ready to quit smoking for good, they should call 1-800-QUITNOW or talk with their doctor about finding the best way to quit using proven methods and FDA-approved treatments and counseling. Are There Risks of Secondhand E-Cigarette Emissions? In 2016, the Surgeon General concluded that secondhand emissions contain, "nicotine; ultrafine particles; flavorings such as diacetyl, a chemical linked to serious lung disease; volatile organic compounds such as benzene, which is found in car exhaust; and heavy metals, such as nickel, tin, and lead."2 Why Isn't More Being Done to Protect Kids from E-Cigarettes? In March, the American Lung Association and our public health partners filed a lawsuit against the Food and Drug Administration challenging its decision that allows electronic cigarettes and cigars—including candy-flavored products that appeal to kids—to stay on the market for years without being reviewed by the agency. The lawsuit contends that the FDA's decision leaves on the market tobacco products that appeal to kids, deprives the FDA and the public of critical information about the health impact of products already on the market, and relieves manufacturers of the burden to produce scientific evidence that their products have a public health benefit.
-
Date: May 26, 2015 Source: American Physiological Society (APS) Summary: With the use of e-cigarettes on the rise, especially among young people, research to uncover the health effects of e-cigs is becoming increasingly important. In a new study, researchers find that e-cig solution and vapors—even those that are nicotine-free—damage lung health. https://www.sciencedaily.com/releases/2015/05/150526084955.htm Electronic cigarette (e-cig) use has now surpassed traditional cigarette use among middle and high school students, according to the Centers for Disease Control and Prevention. This leaves many parents, public health officials and consumers asking whether e-cigarettes are better or worse for lung health than traditional cigarettes. Now, a team of researchers adds its findings to others that suggest nicotine in any form is damaging to lungs. This new research also suggests that non-nicotine-containing e-cig solutions have a damaging effect on lung health, leading researchers to call for more e-cig research. The loss of integrity in the lung endothelial cells -- the cells that make up the lining of the lungs -- can contribute to lung injury and inflammation, but it is unknown what component of cigarette smoke causes lung cells to breakdown. Researchers wrote, "We investigated if nicotine, one of the hundreds of molecules present in [cigarette smoke] extracts, is sufficient to alter lung endothelial barrier function by affecting cytoskeletal regulation," which is the cell's internal matrix that supports cell shape and function. The researchers exposed mice and both human and mouse cells to cigarette smoke and e-cigarette solution that either contained nicotine or was nicotine-free. Their findings shed light on how cigarette smoke damages the lungs and point directly to nicotine as the cause. "Nicotine has dose-dependent deleterious pulmonary effects that result in loss of lung endothelial barrier function, acute lung inflammation and decreased lung endothelial cell proliferation," they wrote. The effects of nicotine were seen both in cigarette smoke and in e-cig solutions that contained nicotine. Interestingly, nicotine-free e-cig solutions were also found to include lung-harming substances, such as acrolein. This substance, which is present in both e-cig solution and vapor, has been shown to damage the lungs by attacking the molecules that hold endothelial cells together. "The increased use of inhaled nicotine via e-cigarettes, especially among the youth, prompts increased research into the effects on health. This research reports that components found in commercially available e-cigarette solutions and vapors generated by heating them may cause lung inflammation," said lead researcher Irina Petrache, PhD. "The effects described characterize short-term effects of e-cig exposures. Whereas studies of long-term effects await further investigations, these results caution that e-cigarette inhalation may be associated with adverse effects on lung health." The article "Endothelial disruptive pro-inflammatory effects of nicotine and e-cigarette vapor exposures" is published ahead of print in the American Journal of Physiology -- Lung Cellular and Molecular Physiology.
-
You might as well work in a coal-fired power plant without any respiratory protection. Good article below. By Alan Mozes HealthDay Reporter https://www.webmd.com/smoking-cessation/news/20180226/toxic-metals-found-in-e-cigarette-vapor#1 MONDAY, Feb. 26, 2018 (HealthDay News) -- If you think that "vaping" is a safe alternative to smoking, new research suggests you might be inadvertently inhaling unsafe levels of toxic metals. Scientists say the tiny metal coils that heat the liquid nitrogen in e-cigarettes may contaminate the resulting vapor with lead, chromium, manganese and nickel. The finding raises the possibility that e-cigarettes are not harmless to users. "We analyzed 15 metals in e-liquid from the refill dispenser -- before the liquid meets the heating element -- in the vapor, and in the remaining e-liquid in the tank after vaping," explained study author Pablo Olmedo. He's an assistant scientist with the Johns Hopkins School of Public Health's department of environmental health and engineering, in Baltimore. "We found that the metal concentrations were generally higher in the tank and aerosol compared to the refill dispenser," said Olmedo. That suggests that the heating coil is the smoking gun, he added. But study co-author Ana Maria Rule pointed out that their team also found "the presence of some metals in some of the liquids even before they are in contact with the coil." That could mean that "in addition to the metal coil, other factors could play a role in e-cigarette metal exposure, such as the voltage used to heat the coil," said Rule, also an assistant scientist at Hopkins. Unlike traditional smoking, vaping works by heating liquids that contain nicotine. The liquid passes through a heating coil, producing a vapor that proponents claim is free of much of the carcinogens associated with burning tobacco leaves. Given that a recent U.S. National Institute on Drug Abuse survey found that one in six high schoolers has vaped in the past month, the finding could have broad public health implications, the researchers said. In the Hopkins study, published Feb. 21 in the journal Environmental Health Perspectives, investigators recruited 56 vapers in the Baltimore area to see whether the heating process introduces toxins into what is inhaled. The researchers used the vapers' own e-cigarette devices when examining the chemical content of e-liquid, vapor and residue. Tested chemicals included: aluminum, antimony, arsenic, cadmium, chromium, copper, iron, lead, manganese, nickel, titanium, tungsten, uranium and zinc. Prior research has linked prolonged inhalation of such metals to lung, liver, heart and brain damage. Chronic exposure may also depress immune system function and raise the risk for certain types of cancer, the researchers said. The team found that e-liquid exposed to heating coils produced a vapor containing significant amounts of chromium, lead, manganese, nickel and zinc. Highly toxic arsenic was also found in both the e-liquid and the heated vapor among a subset of 10 vapers, though how that metal got into the unheated e-liquid remains unclear. The team also noted that toxic metal levels seemed to be higher among vapers who changed their heating coils more often, suggesting that new coils may produce more toxins than older ones. Regardless, Rule said, vapers should know that "as far as we know, all current electronic cigarettes use a metallic coil to generate the vapor, so not vaping is the only way to avoid or mitigate this [toxic] exposure." As for whether vaping is safer than smoking or worse, Rule said the team "did not set out to compare e-cigarettes to cigarettes."
-
- 1
-
-
-
Nicodemon's Lies? by John R. Polito Nicotine Cessation Educator https://whyquit.com/whyquit/A_NicodemonsLies.html Why a question mark behind "Nicodemon's Lies"? Because there is no Nicodemon. Because there are zero monsters or demons within us. It's just another lie, our lie, as dependency ignorance tried to make sense of continued smoking. As teenagers, what most of us thought would be a brief rebellious experiment was quickly transformed into a powerful lifelong chemical addiction as regular nicotine feedings soon became mandatory. Research confirms that for many, it only took a couple of nicotine laden cigarettes before the shackles of slavery started to close. What seemed innocent soon resulted in a brain wanting disorder. Without us realizing it, nicotine was activating, saturating, de-sensitizing and up-regulating dopamine pathway receptors, as our brain's priorities teaching circuitry was taken hostage. Two, five, eight nicotine fixes a day. When will enough be enough? "I'll quit tomorrow" or "I love smoking" became our cry! Welcome to the realities of true chemical dependency. A world built upon lies. Science calls our lies denial. Denial is an unconscious defense mechanism - just below the surface - for resolving the emotional conflict and anxieties that naturally arise from living in a permanent state of self-destructive chemical bondage. Three primary areas of denial relied upon by nicotine addicts are dependency denial, cost denial and recovery denial. Truth is sacrificed for peace of mind, to remain hostage in an artificial world of "nicotine normal," or to justify relapse. Most nicotine addicts we'll see today are fully insulated by a thick blanket of unconscious denial rationalizations, minimization's, fault projections, escapes, intellectualizations and delusions that hide the pain of captivity or create the illusion that the problem is somehow being solved. The average addict musters the courage to say "no" to the wanting for that next fix about once every 2.5 years. It's then that roughly 1 in 20 will succeed in breaking free for an entire year. These horrible recovery statistics eventually result in half of us dying by our own hand, with male smokers losing an average of 13 years of life expectancy, while females lose 14. Our intentional self-destruction is undeniable evidence of the depths of denial. Denial insulates us from the extreme price paid with each and every puff - a little more of life itself. It doesn't have to be. Welcome to WhyQuit, we've been waiting on you! Aside from this article, we've put together a vast array of quality recovery tools to aid you in becoming far smarter than your addiction is strong. They include mind-expanding motivational pages, the Net's largest collection of original quitting articles, quitting tip lists, two free quitting e-books ("Never Take Another Puff" and "Freedom from Nicotine - The Journey Home"), more than 400 free video lessons, and highly focused group support at Turkeyville, our Facebook group. According to the World Health Organization, the next three years will cost 15 million of our brother and sister addicts their lives. Once residing here on Easy Street with us, we hope you'll share what you've learned as failure to either self-discover or be taught the "Law of Addiction" is a horrible reason to die. OUR LIE: My cigarettes are my friend. THE TRUTH: Friend or master? What kind of "friend" would deprive us of oxygen, take away our ability to smell, burn our clothes, destroy our teeth, harden our arteries, elevate our blood pressure, daily feed us 4,000+ chemical compounds that include arsenic, ammonia, acetone, formaldehyde, butane, massive doses of carbon monoxide, hydrogen cyanide, methane, stearic acid, vinyl chloride, mercury, and lead, together with 81 known cancer causing agents (one of which is created when nicotine breaks down - NNK), before finally killing you with cancer, a stroke, a heart attack or emphysema? Imagine seeing your executioner as a friend. Imagine residing inside a mind that is so sick it is willing to trade 13 years of life for one chemical. OUR LIE: I enjoy smoking. THE TRUTH: This may be the most deeply ingrained rationalization of all as it has a solid basis in the following flawed denial logic. "I don't do things that I don't like to do." "I smoke lots and lots of cigarettes." "Therefore, I must really enjoy smoking," instead of the correct conclusion, "therefore, I must really be chemically addicted to smoking nicotine." Did you enjoy being the unaddicted "you" or have you forgotten what it was like to live comfortably inside a mind that does not crave for nicotine? If you cannot remember what it was like being "you" then what basis do you have for honest comparison? If you truly enjoyed being addicted to nicotine then why are you here reading these words? Is it that you liked smoking or that you liked not having to experience what occurred when you didn't smoke - withdrawal? Studies have long ranked nicotine as a more addictive substance than either heroin or cocaine. In fact, cocaine's generally recognized addiction rate among regular users is 15% while nicotine's addiction rate of over 70% is at least five times as great. Imagine convincing your mind that it " likes " being addicted to the drug that addiction scientists now rank as the most addictive substance on all of planet earth. We are nicotine addicts . A pack a day smoker smokes 7,300 cigarettes each and every year. How many of your last 7,300 nicotine fixes did you really enjoy ? How many of the next 7,300 will bring tremendous joy to your life? Isn't it time to be honest? OUR LIE: My spouse, close friend or family member smokes. I'm waiting for them to quit with me. THE TRUTH: Procrastination recovery denial makes the next puff of toxins easier to suck down. Nicotine tells this junkie that they cannot quit until their friend or loved one quits too as they're around their smoke, smells, cigarettes, breath and ashtrays, and quitting is thus impossible. It's pure denial and often both friends or loved ones use the other as their excuse to remain enslaved. How long will you continue to destroy your body while waiting for someone else to quit with you? A lifetime? If and when they do quit with you, what will you do if they relapse? Will "love" cause you to do the same? One of you needs to stand tall and lead the way. It's okay to have hope for a loved one but you must quit for "you" or it's doomed from the very start. Why make your freedom, health or life dependent upon another person's decision. As for being around smokers, it's unavoidable. Should we expect planet earth's 1.2 billion nicotine addicts to disappear once we commence recovery? Won't we still see them and smell their smoke at restaurants, as they stand around outside stores or even hospitals, or as they puff away in the car beside us? Will all the stores pull-down their cigarette displays or move them from arm's reach just because we're trying to reclaim our mind and life? Why live the lie that "I smoke for love!" OUR LIE: It reduces my stress and helps calm me down. THE TRUTH: This stress buster rationalization is false. The body's pH balance is delicate. Nicotine is an alkaloid and stress an acid producing event. The more stressful the event, the quicker the body's remaining nicotine reserves are neutralized (in the same manner as pouring a baking soda solution on an acid covered car battery terminal). The stressed smoker is thrown into early chemical withdrawal adding additional anxiety to the underlying original stressful event. It's why the anxiety associated with a flat tire causes smokers to reach for a cigarette while the non-smoker reaches for a jack. The anxieties build until the doubly stressed smoker cries out "I NEED A CIGARETTE!" Within eight seconds of the first puff, the smoker's nicotine blood serum nicotine level rises and their withdrawal anxieties subside. The addict is left with the false impression that smoking cured the underlying stressful event when in fact the tire is still flat. All non-smokers experience stress too. The difference is that they don't add early nicotine withdrawal to it. In truth, stress nicotine depletion causes smokers to experience far more anxiety than non-smokers. In truth, it is much easier and calmer being the real "you" than it is living as a chemical slave. OUR LIE: My friends smoke, I'll lose them. THE TRUTH: The nicotine smoker's mind has been conditioned to believe, through association, that smoking is central to their entire life. Telephone calls, computer time, work, meals, driving, talking, walking, stress, joy, sorrow, and even romance, may have developed a subconscious association with smoking. The truth is that none of these activities will be altered whatsoever by the absence of tobacco. The truth is that quitting smoking will not deprive you of even a single friend or loved one. The truth is that smoking is costing you new friends and possible relationships as fewer and fewer non-smokers are willing to tolerate being around the smell and the smoke. Can you blame them? With the exception of quitting, your current life doesn't need to change at all unless you want it to change. It might be nice to enlarge your circle of friends to include those who don't stand around the community ashtray, but that's totally up to you. OUR LIE: It wakes me up and keeps me alert. THE TRUTH: This dependency rationalization uses a basic truth (nicotine releases adrenaline and a host of other hormones) to hide the fact that nicotine deprives us of the ability to enjoy prolonged periods of deep conscious relaxation. If always at the peak of alertness because we are addicted to and chemically dependent upon a central nervous system stimulant then when do we truly relax? This dependency rationalization also subverts and ignores a host of natural alertness techniques ranging from a simple deep breath to brief periods of stretching or moderately exhilarating activity. Instead of engaging life on life's terms, a powerful puff of nicotine starts a neurochemical chain-reaction that increases breathing rate, accelerates heart rate, constricts blood vessels, elevates blood pressure, causes the liver to release stored cholesterol into the blood stream, the adrenal gland to release glucocorticoids, the thyroid to release metabolism hormones, the hypothalamus to release corticotropin-releasing hormones, a decrease of progesterone levels in females and testosterone in males, digestive tract shut-down, a glucose release into the bloodstream followed by a boost in insulin to metabolize it, pupil dilation, and your blood to thicken. Inside those highly constricted and over-pressurized blood vessels, carbon monoxide eats away at their teflon like lining (endothelium) while nicotine amazingly vascularizes fat buildups, causing arteries to harden. More smokers die from circulatory disease each year than from lung cancer, yet denial kept almost all of them from wanting to know how or why. What goes up must come down. Once the hormones wear off and that drained feeling begins to arrive, a new puff of nicotine again whips every central nervous system neuron in a tired body like some overworked horse never allowed to rest. Alert, yes, but somewhere in that endless cycle between alert and exhausted resides the "real" you. OUR LIE: My concentration is better. THE TRUTH: Vast quantities of carbon monoxide do NOT improve concentration. Although nicotine is a stimulant and does excite certain brain neurons, it also constricts all blood vessels. Feel how cold your fingers and toes get when deprived of blood flow while smoking. Imagine what's happening to the blood vessels in your brain. If nicotine results in a stroke we probably won't need to worry much about concentration. Fresh air and exercise are far healthier brain stimulants. When quitting it's important that you understand the role that nicotine played in regulating blood sugar as its absence may cause the temporary impairment of concentration and clear thinking. If you are experiencing any concentration problems be sure and drink plenty of fruit juice the first three days if your diet and health permit (cranberry is excellent), as it will help stabilize blood sugars. Also don't skip meals! Nicotine released stored fats into our blood and in a sense fed us with every puff, but not anymore. Don't eat more food each day, just spread your normal intake out more over your entire day so that you keep fuel in your stomach and your blood sugar level. OUR LIE: It's something to do with my hands. THE TRUTH: So is playing with a loaded gun and they both have the same potential for harm. This weak addiction rationalization ignores that doodling with a pen, playing with coins, squeezing a ball or using strength grippers may be habit forming but are non-addictive. You might get ink on yourself, rich or strong wrists but your chances of serious injury or death are almost zero. OUR LIE: My coffee won't be the same. THE TRUTH: More junkie thinking! Your coffee's flavor will remain identical. In fact, it may even taste better once your taste buds heal after years of being numbed, coated and poisoned. Your sense of smell may become so refined that you'll smell fresh coffee brewing more than one hundred feet away. Although you don't need to give up your coffee or any thing else except nicotine during recovery, be aware that nicotine somehow doubles the rate ( 203%) by which caffeine is metabolized by the body. As a new ex-smoker you may only need half as much caffeine in order to obtain the same effect. If you are a heavy caffeine user and find yourself experiencing increased anxiety during recovery, or encounter difficulty sleeping, try reducing your intake by roughly half. OUR LIE: There's lots of time left to quit. THE TRUTH: This year tobacco will kill 5,000,000 humans. Roughly 1 in 4 smokers die in middle-age, each an average of 22.5 years early. In order for 22.5 to be the average, how many hundreds of thousands had to die even younger? Maybe you have plenty of time remaining and maybe not. Dying in your thirties or forties is a powerful price to pay for guessing wrong. The numbers above only reflect DEATH by tobacco. You may be lucky enough to be among the millions of nicotine smokers each year who survive and "only" have a heart attack, a stroke, a lung removed, go onto oxygen, or who receive news of permanent lung disease as they for every breath. Which puff, from which cigarette, in which pack, will pull the trigger that fires the gun? The odds of a male smoker dying from lung cancer are 22 times greater than for a non-smoker. His odds of dying from emphysema are ten times greater. How much longer will your luck hold? OUR LIE: It's one of my few pleasures in life. THE TRUTH: Does that mean that it's better than the pleasure of having a throat to deliver fresh air and great food, two lungs with which to laugh, a healthy heart to feel love, or an undamaged mind which dreams of wonderful tomorrows? Pleasure from your addiction or pleasure in committing slow suicide at the hands of a mind that thinks it can only live with the aid of a powerful stimulant? What do they call someone who derives pleasure from self-inflicted harm or who slowly puts themselves to death? Pick your own label. Which nicotine fix out of the last 5,000 was the one that brought you tremendous pleasure? Which cigarette out of the next 5,000 may be the one that sparks permanent damage or disease, or that carries death's eternal flame? If bad news arrives tomorrow will "pleasure" cross your mind? As for Newport type "pleasure," isn't the real pleasure in satisfying our brain's wanting for more? Now imagine the pleasure of going 72 hours without nicotine, the pride of once again residing inside a nicotine-free body and mind! OUR LIE: Dad just died, this isn't the time! THE TRUTH: Smoking won't bring dad back nor cure any other ill in life. Success in quitting during a period of high stress in life insures that future high stress situations will never again serve as the mind's excuse or justification for relapse. If you think about it, if we continue to live we will all see someone we love die. Such is the cycle of life. Sadly, serious illness, injury, or the death of a loved one are some of the most convincing relapse justifications, the best yet sickest excuses of all to get our drug back. I mean, who would dare question our drug use upon our mother's death? There is no better time to quit than before your next mandatory feeding. In fact, two recent studies found that unplanned quitting attempts are twice as likely to succeed as planned ones (picture quitting day anticipation anxieties slowly eating away and destroying resolve before quitting day ever arrives). Why allow finances, work, illness, education or relationships to serve as an excuse to remain an active addict? Once free, there is no legitimate justification for ever putting nicotine back into our body - none, zero, never! OUR LIE: Lots of smokers live until ripe old age. THE TRUTH: They are much rarer than you think. Look around. If you do find old nicotine smokers almost all are in poor health or in advanced stages of smoking related diseases, many with oxygen. Laboring for every breath with lungs on their last leg, is that ripe enough for us? Nicotine smokers tend to think only in terms of dying from lung cancer. Tobacco kills in many ways. For example, circulatory disease caused by smoking kills more smokers each year than lung cancer. How long would George Burns have lived to be if he hadn't smoked cigars, 115, 125? Click here to look at the " truth ". What's wrong with dying healthy from natural causes! OUR LIE: I get bored. It helps pass the time. THE TRUTH: Tobacco does not control any clock on earth but it does control you . For the pack a day nicotine smoker it takes about 30 minutes before their blood serum nicotine level drops to the point where their mind sends them an "urge" of discomfort to remind you that it's time for a feeding. It doesn't matter where they are or what they're doing. Depending upon your daily nicotine requirements, the voice inside your head will let you know when it's time. All you're doing when bored is being alert to what lies ahead, so that you keep topping off your nicotine tank before the next urge arrives. Boredom is supposed to be a positive form of anxiety that motivates us to accomplish a task that hopefully helps preserve life, not destroy it. OUR LIE: It's my choice and I choose to smoke! THE TRUTH: It's a lie and you know it! We lost all "choice" and the ability to simply walk away the day that nicotine feedings became mandatory. The only choices now are to either arrest our dependency or to decide how early and often we'll feed it. As harsh as this sounds, nicotine dependency is a brain wanting disorder, a true mental illness. But the ignorant nicotine addict still believes the "choice" myth pounded into their brain by an endless stream of highly effective tobacco company marketing. All the pretty colored boxes, the displays, the sea of store ads, they make it seem like we can't wait to wake-up each day and run down to the store and try a new brand. Although a well set trap for gullible children and teens who can't wait to become adults, it also makes quitting more challenging than need be. The uneducated smoker likely associates smoking with reading the newspaper, coffee, travel, stress, other smokers, telephone calls, meals, celebrations, romance, or even as a necessary step prior to walking into a store. The educated nicotine addict sees all nicotine fixes as either mandatory, or an early feeding, in order to avoid the onset and discomfort of chemical withdrawal. We smoked after a meal because it was once again time for a nicotine feeding. We smoked before the meal because we didn't know how long eating would last and it isn't polite to eat and smoke at the same time. If your regular feedings are spaced thirty minutes apart, at least every thirty minutes you're going to start sensing growing want for more nicotine regardless of the activity. OUR LIE: I'm only hurting me. THE TRUTH: Have you stopped for even one moment to reflect upon the financial, physical or emotional pain that your needless dying and death will bring your loved ones? Do we care that the deadly byproducts of our addiction have the potential to harm or kill family members, whose only crime was loving us? According to the World Health Organization secondhand smoke contributes to causing lower respiratory tract infections such as pneumonia and bronchitis, colds, coughing, wheezing, worsening of asthma, middle ear disease, cardiovascular disease, and even neuro-behavioral impairment (especially in young children). It also found that maternal smoking or exposure to second-hand smoke during pregnancy is a major cause of sudden infant death syndrome (SIDS), reduced birth weight and decreased lung function. How much does it cost to attempt to cure mouth, throat or lung cancer? $100,000? $200,000? $300,000? What's the cost of a funeral today and which loved one have you designated to pay the emotional price of making arrangements for your early departure? What about the loss to loved ones of our guidance, our help around the house or any income we contribute? Where will they turn? OUR LIE: A cure for cancer is coming soon. THE TRUTH: Between Europe and North America tobacco will kill over one million this year. How many of them thought that a cure was on the way? Sadly, it was false hope. As hopeless drug addicts they waited, and waited and waited. What type of lung cancer are hoping they'll cure - squamous cell, oat cell, adenocarcinoma, or one of the less common forms of lung cancer? Even if a cure is coming for all forms and types of cancer caused by tobacco (and there are many), what will be left of your lungs by the time it arrives? If you're gambling on "how" tobacco will kill you, don't forget to consider heart attacks, strokes, and emphysema. Which cure are you betting on? OUR LIE: I smoke lights and they're not as bad. THE TRUTH: Lights, ultra-lights and milds are often capable of delivering the same amount of tar and nicotine as regular brands, depending on how they're smoked. It's why use of those terms are being banned by governments. They do not reduce most health risks including the risk of heart disease or the risk of cancer. In fact, their smokers often take longer drags which means more tar and more nicotine than advertised. Others simply smoke a greater number of lights because they feel short changed. OUR LIE: It's my right to blow smoke! THE TRUTH: And it's the right of non-smokers and ex-smokers to be free from your smoke too. Social controls to protect the rights of non-smokers are now sweeping the globe. Can a dog's life-span be cut in half by a smoking master? Would you intentionally double the risk of heart attack or triple the risk of lung cancer for a spouse or family member? Why kill the innocent too? Are non-smokers who get extremely upset at having to breathe side-stream smoke simply being obnoxious or are they fighting to protect themselves and those they love from the known harms generated from burning a plant that contains 44 known cancer causing agents and releases 4,000+ chemical compounds when burned? Do you know a child whose mother smoked while pregnant, who does not suffer from some form of impairment today? Look closely. OUR LIE: Quitting causes weight gain and it's just as dangerous. THE TRUTH: This intellectual denial pre-assumes a large weight gain and then makes an erroneous judgment regarding relative risks. Quitting does not increase our weight, eating does. Some assert that metabolic changes associated primarily with the heart not having to work as hard could account for a pound or two but as far as being " dangerous," you'd have to gain at least 75 additional pounds in order to equal the health risks associated with smoking one pack a day. Keep in mind that your general health, physical abilities and lung capacity will all improve dramatically. If patient, you will soon regain the ability to build cardiovascular endurance, and experience up to a 30% increase in overall lung function within 90 days. You'll be able to apply the same mental recovery tools needed to take control of your addiction in shedding any extra pounds, just one pound at a time. Remember, smoking was your cue that a meal had ended. Unless you develop a new healthy cue there may be fewer leftovers. Also keep in mind how easy it would be for a drug addict to use intentional weight gain to a ploy to sabotage recovery. Additionally, nicotine stimulated brain dopamine pathways and so does food. Be careful not to use food as a destructive dopamine replacement crutch. If at all concerned, consider having a supply of fresh fruits and veggies cut up, handy and ready to eat during the 2-3 weeks it takes the brain to restore natural dopamine pathway sensitivities. OUR LIE: It's too late now to heal these lungs. THE TRUTH: Nonsense! While true that each and every puff destroyed more of each lung's roughly 300 million air sacs (alveoli), we were each blessed with millions more than needed to live a full and complete life. It's amazing how much damaged lungs can repair themselves unless disease or cancer has already arrived. Even with emphysema, although destroyed air sacks will never again function, quitting now will immediately halt the needless destruction of additional sacs. You only have two options - decay or heal, including the possibility of experiencing up to a 30 percent increase in overall lung function within 90 days of quitting. If continuing assault by the 81 cancer causing chemicals so far identified in cigarette smoke, which cigarette in which pack contains the spark that gives birth to that first cancerous cell? OUR LIE: I'd quit but withdrawal never ends! THE TRUTH: Hogwash! If you remain 100% nicotine free for just 72 hours your blood will become nicotine free, your withdrawal anxieties will peak in intensity and the number of psychological craves will peak in number. The greatest challenge will be over. Actual physical withdrawal will be complete within 2-3 weeks as the brain re-sensitizes dopamine pathway receptors and down-regulates their numbers to levels seen in non-smokers. During that time you'll encounter and recondition (extinguish) all but remote or seasonal psychological habit crave triggers and begin to witness the gradually diminishing influence of thousands of nicotine replenishment memories, memories that belonged to an actively feeding addict who once again was in need of a fix. If you focus on taking recovery just one hour, challenge and day at a time, before you know it you'll experience your first day of total comfort, where never once do you think about wanting to smoke nicotine. I call it a silent celebration because you probably won't even realize that it has happened until the next day. After the first such day, they grow more and more frequent until they become your new sense of normal. If just starting out, the rich and deep sense of comfort and calm that awaits you is beyond your enslaved mind's ability to comprehension. Why? Because your dopamine pathways, your mind's priorities teacher, have been hijacked, making that next nicotine fix as important as eating food. Food craves, nicotine craves but with one critical difference. Without food we die. Without nicotine we thrive. It's why, although as real as your name, you cannot trust the nicotine wanting message that pounds inside your head, as it is false and is destroying you. OUR LIE: But the craves last for hours! THE TRUTH: Just like the lingering thought of a nice juicy steak, lobster in butter sauce, or fresh baked hot apple pie, you can make yourself "think" about having a cigarette all day long, if that's what you really want to do. Unlike fixating on a conscious thought about smoking, subconsciously cue triggered crave anxiety attacks almost always last for less than 3 minutes. But it's important that you look at a clock and time the crave episode as cessation time distortion (a normal and expected recovery symptom) can make minutes feel like hours. The good news is that most of the anxiety surrounding crave episodes is self induced and thus controllable. Key is in not trying to hide or run from your mind's junkie thinking but exposing it to honest analysis and positive thinking. Strip away all the self-inflicted anxiety and at worst, what remains on quitting day 3 for the "average" quitter is just 18 minutes of true crave anxiety (an average of six craves, each less than three minutes in duration). OUR LIE: I'll quit after the next pack, next carton, next month, my next birthday or New Years. THE TRUTH: Oh really? Can you count on both hands and all your toes how many times you've lied to yourself with such nonsense? And which pack, carton, month or birthday will give you the best chance for success? Forget buying nicotine laden cigarettes by the pack or carton. A case is even cheaper! With the way that cigarette prices are shooting through the roof, you might as well calculate how many it will take to keep you in nicotine for life and buy them all now. The only problem with that is in determining how long you have left to live. How many more pack, carton, birthday and New Year's lies will you tell to yourself? When will they stop? If you continue on your present path, many Birthdays will likely be canceled by a rather early Deathday. You are a true drug addict in every sense and the "wanting" inside your brain is as real as the greatest truth you know. What isn't true is the message, that that next fix is important. Truth is, everything now done under nicotine's influence can be done as well as or better without it. OUR LIE: I like to smoke when I drink and I find myself smoking even more. THE TRUTH: The effects of drinking and stress upon our body's nicotine level are nearly the same. You smoke more when you drink not because you "like" to but because you MUST. Like stress, alcohol is an acid producing event that causes urine to become more acidic. The greater the acid level of urine, the quicker our kidneys remove and eliminate nicotine reserves from the bloodstream. Thus, the more you drink, the more nicotine you'll need to smoke or ingest in order to avoid sensing the onset of the anxiety of early withdrawal. Although early alcohol use contributes to destroying a great many quit attempts, understanding the nicotine-acid relationship can be of benefit in accelerating physical nicotine withdrawal so that quitters can begin feeling relief sooner. Acidic fruit juices, such as cranberry, may help reduce the normal 72 hours of withdrawal required to remove all nicotine from the blood. In that roughly 50% of all relapses are associated with alcohol use, if at all possible don't drink during the first few days of recovery. When you do decide to drink, consider drinking at home first without cigarettes around before testing your resolve around smokers. By doing so you'll help to break the your mind's psychological links between smoking and drinking with as little risk as possible. As millions of ex-smokers can attest, your beer or drink will taste better than ever once your taste buds are allowed an opportunity to heal. OUR LIE: It's too painful to quit! THE TRUTH: Compared to what? Three days of physical withdrawal (just 72 hours) in no way compares to the pain of months of chemotherapy, lung removal surgery and a two foot scar, a losing battle with throat cancer, years of trying to recover from a serious stroke or massive heart attack, or fighting for every breath through emphysema riddled lungs as you drag oxygen around for the balance of life. If you're really worried about hurt then why continue your daily destruction? OUR LIE: If I quit, I'll just start back again. I always do. THE TRUTH: The truth is that you do not have to relapse. We relapse because we rewrite the Law of Addiction, we forget why we quit, or we invent lies and stupid excuses, such as those that fill this page. Your next quit can be your last but you need to learn how to care for your recovery, while always applying the only rule that you'll ever need to obey - to NEVER TAKE ANOTHER PUFF! OUR LIE: I'll cut down or quit and smoke just one now and then. THE TRUTH: It's every addict's dream, to control the uncontrollable. You are addicted to a substance that is five times as addictive as powdered cocaine (15% vs. 75%). You may be strong enough to cut back but so long as nicotine continues to arrive you'll remain hooked, the decay will continue, and as studies suggest, even though smoking less your health risks will remain almost unchanged. If you were a pack-a-day nicotine smoker and after quitting you decide to smoke just one cigarette, you might as well get ready to smoke the other 7,300 for the year too as full and complete relapse is virtually assured. The Law of Addiction is simple - just one puff of new nicotine and it's over. Brain scans show that up to 50% of dopamine pathway receptors become occupied by nicotine within eight seconds of the first puff. While roughly half walk away from relapse totally convinced that they've gotten away with smoking just once, they've saturated and de-sensitized dopamine pathway receptors and will soon find their brain begging for more. You see, as permanent as alcoholism, once hooked we somehow stay hard wired for relapse for the balance of life. Although recovery allows the brain time to heal and function normally again the tracks of addiction remain. We cannot cure or kill our disease. Once free, we remain on probation for the balance of life. OUR LIE: I tried quitting but my family stopped supporting me or was giving me such a hard time that it caused me to throw in the towel. THE TRUTH: It's a lie. You gave up because you used your family as a cheap excuse to get your drug back. You exaggerated everything they did or didn't do. You were looking for any excuse. You're the drug addict yet you expected them to understand the weakness and thinking of a drug addict's mind. Maybe they didn't pat you on the back as often as you wanted, but is it really fair to expect them to appreciate the magnitude or duration of your challenge if they've never been through chemical withdrawal themselves? They just want you to be normal. They don't know how to react. Do they pat you on the back and keep reminding you, or hope and pray that the worst has already passed? Feeling unappreciated, picking fights and creating confrontation are tools of the addict's mind that are often used as weapons in order to reclaim their drug. Some know that if they inflict tremendous stress on loved ones that they may even convince their loved one to beg them to start smoking nicotine again, or better yet, to go buy their relapse cigarettes for them. That way, they can blame their relapse on their loved one. "They just couldn't handle my quitting." "Maybe next time!" The lengths to which we'll go in order to feed our wanting are almost beyond belief. Yes, some of us will even hurt those that love us most. OUR LIE: OK, I'm going to stop! Now I can enjoy my smokes until then! THE TRUTH: If you've done this more than once, isn't it just more junkie head games? This addict wants to feel good about smoking nicotine and they've learned that by saying that they're going to quit, that they make themselves feel better even though deep down they know that it's probably just another lie! Unless something awakens this addict, there may never be a serious quit in their future. OUR LIE: I've got to die of something! THE TRUTH: True, but if you knew that tomorrow morning at 9:22 a.m. a massive smoking induced stroke would bring your life to an abrupt end, and you'd die on a cold floor with a cigarette beside you - just as tens of thousands of smokers are found each year? Would you light that last cigarette at 9:21 a.m. and pull the trigger that kills you? Is this one of your primary use rationalizations? Look around at all the smokers you see today. The death certificates of half will read, "cause of death - smoking." Yes, they had to die of something but not an average of more than 5,000 days early. Have you met Noni, Bryan, Deb and Kim? Would any non-addicted human spend each and every day of the remainder of their life intentionally destroying more of their body's ability to receive and transport life giving oxygen? Would they continue doing so until physical exercise was no longer an option, or until this mental illness called dependency forced others to begin caring for us, as they watch us struggle just to suck oxygen from tanks and machines? Which family member have you prepared to be your care giver? Try to imagine what it's like to breathe through a straw? It's called emphysema. Why not find a straw and give it a try. What has nicotine done for you lately? OUR LIE: I can't quit alone. I'll need nicotine gum, the patch, hypnosis, e-cigs, acupuncture, magic herbs or other wonder drugs! THE TRUTH: Wrong! The simple truth is that no magic cure has ever "made" any smoker quit smoking nicotine. The key to immediate and lasting abstinence is education and understanding, in becoming vastly more dependency recovery savvy than our addiction is strong. Hypnosis and acupuncture teach us nothing, nor does use of nicotine replacement products that fail roughly 93% of users within 6 months of quitting, while making NRT slaves of a substantial percentage of those who actually quit smokings. What quitting product and procedure salesmen will never tell you is that each year cold turkey generates more successful long-term ex-users than all other quitting methods combined. Why? Because they want your money. Remember, should all else fail, you always have you! OUR LIE: It's all Nicodemon's fault, not mine! THE TRUTH: There is no Nicodemon, no little monsters, no big monsters, no monsters at all. None! In fact, the title to this article, Nicodemon's Lies, is one of the biggest lies of all. They were never Nicodemon's lies but our lies. Nicotine is simply a chemical, a drug, an alkaloid known as C10H14N2. Its I.Q. is and always has been zero. It does not think, plan, inflict punishment, nor will it conspire to make you relapse or die addicted to it. The fact that it has zero intelligence has always been your greatest weapon. Everything you see, feel, and sense during nicotine withdrawal and recovery will be grounded in chemical dependency, conditioning, reason, logic, emotion or science. Any conspirators in any past attempts to make you relapse and destroy your recovery were always and only "you!" Never once did you relapse due to external circumstances. It was 100% internal, once again you introduced nicotine into your bloodstream. The good news is that while each defeat was yours, so too will be the victory. Should you end nicotine's control of your brain's reward pathways the victory will belong only to you!
- 5 replies
-
- 12
-
-
-
- truths
- rationalization
- (and 4 more)
-
...Science calls our lies denial. Denial is an unconscious defense mechanism - just below the surface - for resolving the emotional conflict and anxieties that naturally arise from living in a permanent state of self-destructive chemical bondage. Nicodemon's Lies? by John R. Polito Nicotine Cessation Educator https://whyquit.com/whyquit/A_NicodemonsLies.html Why a question mark behind "Nicodemon's Lies"? Because there is no Nicodemon. Because there are zero monsters or demons within us. It's just another lie, our lie, as dependency ignorance tried to make sense of continued smoking. As teenagers, what most of us thought would be a brief rebellious experiment was quickly transformed into a powerful lifelong chemical addiction as regular nicotine feedings soon became mandatory. Research confirms that for many, it only took a couple of nicotine laden cigarettes before the shackles of slavery started to close. What seemed innocent soon resulted in a brain wanting disorder. Without us realizing it, nicotine was activating, saturating, de-sensitizing and up-regulating dopamine pathway receptors, as our brain's priorities teaching circuitry was taken hostage. Two, five, eight nicotine fixes a day. When will enough be enough? "I'll quit tomorrow" or "I love smoking" became our cry! Welcome to the realities of true chemical dependency. A world built upon lies. Science calls our lies denial. Denial is an unconscious defense mechanism - just below the surface - for resolving the emotional conflict and anxieties that naturally arise from living in a permanent state of self-destructive chemical bondage. Three primary areas of denial relied upon by nicotine addicts are dependency denial, cost denial and recovery denial. Truth is sacrificed for peace of mind, to remain hostage in an artificial world of "nicotine normal," or to justify relapse. Most nicotine addicts we'll see today are fully insulated by a thick blanket of unconscious denial rationalizations, minimization's, fault projections, escapes, intellectualizations and delusions that hide the pain of captivity or create the illusion that the problem is somehow being solved. The average addict musters the courage to say "no" to the wanting for that next fix about once every 2.5 years. It's then that roughly 1 in 20 will succeed in breaking free for an entire year. These horrible recovery statistics eventually result in half of us dying by our own hand, with male smokers losing an average of 13 years of life expectancy, while females lose 14. Our intentional self-destruction is undeniable evidence of the depths of denial. Denial insulates us from the extreme price paid with each and every puff - a little more of life itself. It doesn't have to be. Welcome to WhyQuit, we've been waiting on you! Aside from this article, we've put together a vast array of quality recovery tools to aid you in becoming far smarter than your addiction is strong. They include mind-expanding motivational pages, the Net's largest collection of original quitting articles, quitting tip lists, two free quitting e-books ("Never Take Another Puff" and "Freedom from Nicotine - The Journey Home"), more than 400 free video lessons, and highly focused group support at Turkeyville, our Facebook group. According to the World Health Organization, the next three years will cost 15 million of our brother and sister addicts their lives. Once residing here on Easy Street with us, we hope you'll share what you've learned as failure to either self-discover or be taught the "Law of Addiction" is a horrible reason to die. OUR LIE: My cigarettes are my friend. THE TRUTH: Friend or master? What kind of "friend" would deprive us of oxygen, take away our ability to smell, burn our clothes, destroy our teeth, harden our arteries, elevate our blood pressure, daily feed us 4,000+ chemical compounds that include arsenic, ammonia, acetone, formaldehyde, butane, massive doses of carbon monoxide, hydrogen cyanide, methane, stearic acid, vinyl chloride, mercury, and lead, together with 81 known cancer causing agents (one of which is created when nicotine breaks down - NNK), before finally killing you with cancer, a stroke, a heart attack or emphysema? Imagine seeing your executioner as a friend. Imagine residing inside a mind that is so sick it is willing to trade 13 years of life for one chemical. OUR LIE: I enjoy smoking. THE TRUTH: This may be the most deeply ingrained rationalization of all as it has a solid basis in the following flawed denial logic. "I don't do things that I don't like to do." "I smoke lots and lots of cigarettes." "Therefore, I must really enjoy smoking," instead of the correct conclusion, "therefore, I must really be chemically addicted to smoking nicotine." Did you enjoy being the unaddicted "you" or have you forgotten what it was like to live comfortably inside a mind that does not crave for nicotine? If you cannot remember what it was like being "you" then what basis do you have for honest comparison? If you truly enjoyed being addicted to nicotine then why are you here reading these words? Is it that you liked smoking or that you liked not having to experience what occurred when you didn't smoke - withdrawal? Studies have long ranked nicotine as a more addictive substance than either heroin or cocaine. In fact, cocaine's generally recognized addiction rate among regular users is 15% while nicotine's addiction rate of over 70% is at least five times as great. Imagine convincing your mind that it " likes " being addicted to the drug that addiction scientists now rank as the most addictive substance on all of planet earth. We are nicotine addicts . A pack a day smoker smokes 7,300 cigarettes each and every year. How many of your last 7,300 nicotine fixes did you really enjoy ? How many of the next 7,300 will bring tremendous joy to your life? Isn't it time to be honest? OUR LIE: My spouse, close friend or family member smokes. I'm waiting for them to quit with me. THE TRUTH: Procrastination recovery denial makes the next puff of toxins easier to suck down. Nicotine tells this junkie that they cannot quit until their friend or loved one quits too as they're around their smoke, smells, cigarettes, breath and ashtrays, and quitting is thus impossible. It's pure denial and often both friends or loved ones use the other as their excuse to remain enslaved. How long will you continue to destroy your body while waiting for someone else to quit with you? A lifetime? If and when they do quit with you, what will you do if they relapse? Will "love" cause you to do the same? One of you needs to stand tall and lead the way. It's okay to have hope for a loved one but you must quit for "you" or it's doomed from the very start. Why make your freedom, health or life dependent upon another person's decision. As for being around smokers, it's unavoidable. Should we expect planet earth's 1.2 billion nicotine addicts to disappear once we commence recovery? Won't we still see them and smell their smoke at restaurants, as they stand around outside stores or even hospitals, or as they puff away in the car beside us? Will all the stores pull-down their cigarette displays or move them from arm's reach just because we're trying to reclaim our mind and life? Why live the lie that "I smoke for love!" OUR LIE: It reduces my stress and helps calm me down. THE TRUTH: This stress buster rationalization is false. The body's pH balance is delicate. Nicotine is an alkaloid and stress an acid producing event. The more stressful the event, the quicker the body's remaining nicotine reserves are neutralized (in the same manner as pouring a baking soda solution on an acid covered car battery terminal). The stressed smoker is thrown into early chemical withdrawal adding additional anxiety to the underlying original stressful event. It's why the anxiety associated with a flat tire causes smokers to reach for a cigarette while the non-smoker reaches for a jack. The anxieties build until the doubly stressed smoker cries out "I NEED A CIGARETTE!" Within eight seconds of the first puff, the smoker's nicotine blood serum nicotine level rises and their withdrawal anxieties subside. The addict is left with the false impression that smoking cured the underlying stressful event when in fact the tire is still flat. All non-smokers experience stress too. The difference is that they don't add early nicotine withdrawal to it. In truth, stress nicotine depletion causes smokers to experience far more anxiety than non-smokers. In truth, it is much easier and calmer being the real "you" than it is living as a chemical slave. OUR LIE: My friends smoke, I'll lose them. THE TRUTH: The nicotine smoker's mind has been conditioned to believe, through association, that smoking is central to their entire life. Telephone calls, computer time, work, meals, driving, talking, walking, stress, joy, sorrow, and even romance, may have developed a subconscious association with smoking. The truth is that none of these activities will be altered whatsoever by the absence of tobacco. The truth is that quitting smoking will not deprive you of even a single friend or loved one. The truth is that smoking is costing you new friends and possible relationships as fewer and fewer non-smokers are willing to tolerate being around the smell and the smoke. Can you blame them? With the exception of quitting, your current life doesn't need to change at all unless you want it to change. It might be nice to enlarge your circle of friends to include those who don't stand around the community ashtray, but that's totally up to you. OUR LIE: It wakes me up and keeps me alert. THE TRUTH: This dependency rationalization uses a basic truth (nicotine releases adrenaline and a host of other hormones) to hide the fact that nicotine deprives us of the ability to enjoy prolonged periods of deep conscious relaxation. If always at the peak of alertness because we are addicted to and chemically dependent upon a central nervous system stimulant then when do we truly relax? This dependency rationalization also subverts and ignores a host of natural alertness techniques ranging from a simple deep breath to brief periods of stretching or moderately exhilarating activity. Instead of engaging life on life's terms, a powerful puff of nicotine starts a neurochemical chain-reaction that increases breathing rate, accelerates heart rate, constricts blood vessels, elevates blood pressure, causes the liver to release stored cholesterol into the blood stream, the adrenal gland to release glucocorticoids, the thyroid to release metabolism hormones, the hypothalamus to release corticotropin-releasing hormones, a decrease of progesterone levels in females and testosterone in males, digestive tract shut-down, a glucose release into the bloodstream followed by a boost in insulin to metabolize it, pupil dilation, and your blood to thicken. Inside those highly constricted and over-pressurized blood vessels, carbon monoxide eats away at their teflon like lining (endothelium) while nicotine amazingly vascularizes fat buildups, causing arteries to harden. More smokers die from circulatory disease each year than from lung cancer, yet denial kept almost all of them from wanting to know how or why. What goes up must come down. Once the hormones wear off and that drained feeling begins to arrive, a new puff of nicotine again whips every central nervous system neuron in a tired body like some overworked horse never allowed to rest. Alert, yes, but somewhere in that endless cycle between alert and exhausted resides the "real" you. OUR LIE: My concentration is better. THE TRUTH: Vast quantities of carbon monoxide do NOT improve concentration. Although nicotine is a stimulant and does excite certain brain neurons, it also constricts all blood vessels. Feel how cold your fingers and toes get when deprived of blood flow while smoking. Imagine what's happening to the blood vessels in your brain. If nicotine results in a stroke we probably won't need to worry much about concentration. Fresh air and exercise are far healthier brain stimulants. When quitting it's important that you understand the role that nicotine played in regulating blood sugar as its absence may cause the temporary impairment of concentration and clear thinking. If you are experiencing any concentration problems be sure and drink plenty of fruit juice the first three days if your diet and health permit (cranberry is excellent), as it will help stabilize blood sugars. Also don't skip meals! Nicotine released stored fats into our blood and in a sense fed us with every puff, but not anymore. Don't eat more food each day, just spread your normal intake out more over your entire day so that you keep fuel in your stomach and your blood sugar level. OUR LIE: It's something to do with my hands. THE TRUTH: So is playing with a loaded gun and they both have the same potential for harm. This weak addiction rationalization ignores that doodling with a pen, playing with coins, squeezing a ball or using strength grippers may be habit forming but are non-addictive. You might get ink on yourself, rich or strong wrists but your chances of serious injury or death are almost zero. OUR LIE: My coffee won't be the same. THE TRUTH: More junkie thinking! Your coffee's flavor will remain identical. In fact, it may even taste better once your taste buds heal after years of being numbed, coated and poisoned. Your sense of smell may become so refined that you'll smell fresh coffee brewing more than one hundred feet away. Although you don't need to give up your coffee or any thing else except nicotine during recovery, be aware that nicotine somehow doubles the rate ( 203%) by which caffeine is metabolized by the body. As a new ex-smoker you may only need half as much caffeine in order to obtain the same effect. If you are a heavy caffeine user and find yourself experiencing increased anxiety during recovery, or encounter difficulty sleeping, try reducing your intake by roughly half. OUR LIE: There's lots of time left to quit. THE TRUTH: This year tobacco will kill 5,000,000 humans. Roughly 1 in 4 smokers die in middle-age, each an average of 22.5 years early. In order for 22.5 to be the average, how many hundreds of thousands had to die even younger? Maybe you have plenty of time remaining and maybe not. Dying in your thirties or forties is a powerful price to pay for guessing wrong. The numbers above only reflect DEATH by tobacco. You may be lucky enough to be among the millions of nicotine smokers each year who survive and "only" have a heart attack, a stroke, a lung removed, go onto oxygen, or who receive news of permanent lung disease as they for every breath. Which puff, from which cigarette, in which pack, will pull the trigger that fires the gun? The odds of a male smoker dying from lung cancer are 22 times greater than for a non-smoker. His odds of dying from emphysema are ten times greater. How much longer will your luck hold? OUR LIE: It's one of my few pleasures in life. THE TRUTH: Does that mean that it's better than the pleasure of having a throat to deliver fresh air and great food, two lungs with which to laugh, a healthy heart to feel love, or an undamaged mind which dreams of wonderful tomorrows? Pleasure from your addiction or pleasure in committing slow suicide at the hands of a mind that thinks it can only live with the aid of a powerful stimulant? What do they call someone who derives pleasure from self-inflicted harm or who slowly puts themselves to death? Pick your own label. Which nicotine fix out of the last 5,000 was the one that brought you tremendous pleasure? Which cigarette out of the next 5,000 may be the one that sparks permanent damage or disease, or that carries death's eternal flame? If bad news arrives tomorrow will "pleasure" cross your mind? As for Newport type "pleasure," isn't the real pleasure in satisfying our brain's wanting for more? Now imagine the pleasure of going 72 hours without nicotine, the pride of once again residing inside a nicotine-free body and mind! OUR LIE: Dad just died, this isn't the time! THE TRUTH: Smoking won't bring dad back nor cure any other ill in life. Success in quitting during a period of high stress in life insures that future high stress situations will never again serve as the mind's excuse or justification for relapse. If you think about it, if we continue to live we will all see someone we love die. Such is the cycle of life. Sadly, serious illness, injury, or the death of a loved one are some of the most convincing relapse justifications, the best yet sickest excuses of all to get our drug back. I mean, who would dare question our drug use upon our mother's death? There is no better time to quit than before your next mandatory feeding. In fact, two recent studies found that unplanned quitting attempts are twice as likely to succeed as planned ones (picture quitting day anticipation anxieties slowly eating away and destroying resolve before quitting day ever arrives). Why allow finances, work, illness, education or relationships to serve as an excuse to remain an active addict? Once free, there is no legitimate justification for ever putting nicotine back into our body - none, zero, never! OUR LIE: Lots of smokers live until ripe old age. THE TRUTH: They are much rarer than you think. Look around. If you do find old nicotine smokers almost all are in poor health or in advanced stages of smoking related diseases, many with oxygen. Laboring for every breath with lungs on their last leg, is that ripe enough for us? Nicotine smokers tend to think only in terms of dying from lung cancer. Tobacco kills in many ways. For example, circulatory disease caused by smoking kills more smokers each year than lung cancer. How long would George Burns have lived to be if he hadn't smoked cigars, 115, 125? Click here to look at the " truth ". What's wrong with dying healthy from natural causes! OUR LIE: I get bored. It helps pass the time. THE TRUTH: Tobacco does not control any clock on earth but it does control you . For the pack a day nicotine smoker it takes about 30 minutes before their blood serum nicotine level drops to the point where their mind sends them an "urge" of discomfort to remind you that it's time for a feeding. It doesn't matter where they are or what they're doing. Depending upon your daily nicotine requirements, the voice inside your head will let you know when it's time. All you're doing when bored is being alert to what lies ahead, so that you keep topping off your nicotine tank before the next urge arrives. Boredom is supposed to be a positive form of anxiety that motivates us to accomplish a task that hopefully helps preserve life, not destroy it. OUR LIE: It's my choice and I choose to smoke! THE TRUTH: It's a lie and you know it! We lost all "choice" and the ability to simply walk away the day that nicotine feedings became mandatory. The only choices now are to either arrest our dependency or to decide how early and often we'll feed it. As harsh as this sounds, nicotine dependency is a brain wanting disorder, a true mental illness. But the ignorant nicotine addict still believes the "choice" myth pounded into their brain by an endless stream of highly effective tobacco company marketing. All the pretty colored boxes, the displays, the sea of store ads, they make it seem like we can't wait to wake-up each day and run down to the store and try a new brand. Although a well set trap for gullible children and teens who can't wait to become adults, it also makes quitting more challenging than need be. The uneducated smoker likely associates smoking with reading the newspaper, coffee, travel, stress, other smokers, telephone calls, meals, celebrations, romance, or even as a necessary step prior to walking into a store. The educated nicotine addict sees all nicotine fixes as either mandatory, or an early feeding, in order to avoid the onset and discomfort of chemical withdrawal. We smoked after a meal because it was once again time for a nicotine feeding. We smoked before the meal because we didn't know how long eating would last and it isn't polite to eat and smoke at the same time. If your regular feedings are spaced thirty minutes apart, at least every thirty minutes you're going to start sensing growing want for more nicotine regardless of the activity. OUR LIE: I'm only hurting me. THE TRUTH: Have you stopped for even one moment to reflect upon the financial, physical or emotional pain that your needless dying and death will bring your loved ones? Do we care that the deadly byproducts of our addiction have the potential to harm or kill family members, whose only crime was loving us? According to the World Health Organization secondhand smoke contributes to causing lower respiratory tract infections such as pneumonia and bronchitis, colds, coughing, wheezing, worsening of asthma, middle ear disease, cardiovascular disease, and even neuro-behavioral impairment (especially in young children). It also found that maternal smoking or exposure to second-hand smoke during pregnancy is a major cause of sudden infant death syndrome (SIDS), reduced birth weight and decreased lung function. How much does it cost to attempt to cure mouth, throat or lung cancer? $100,000? $200,000? $300,000? What's the cost of a funeral today and which loved one have you designated to pay the emotional price of making arrangements for your early departure? What about the loss to loved ones of our guidance, our help around the house or any income we contribute? Where will they turn? OUR LIE: A cure for cancer is coming soon. THE TRUTH: Between Europe and North America tobacco will kill over one million this year. How many of them thought that a cure was on the way? Sadly, it was false hope. As hopeless drug addicts they waited, and waited and waited. What type of lung cancer are hoping they'll cure - squamous cell, oat cell, adenocarcinoma, or one of the less common forms of lung cancer? Even if a cure is coming for all forms and types of cancer caused by tobacco (and there are many), what will be left of your lungs by the time it arrives? If you're gambling on "how" tobacco will kill you, don't forget to consider heart attacks, strokes, and emphysema. Which cure are you betting on? OUR LIE: I smoke lights and they're not as bad. THE TRUTH: Lights, ultra-lights and milds are often capable of delivering the same amount of tar and nicotine as regular brands, depending on how they're smoked. It's why use of those terms are being banned by governments. They do not reduce most health risks including the risk of heart disease or the risk of cancer. In fact, their smokers often take longer drags which means more tar and more nicotine than advertised. Others simply smoke a greater number of lights because they feel short changed. OUR LIE: It's my right to blow smoke! THE TRUTH: And it's the right of non-smokers and ex-smokers to be free from your smoke too. Social controls to protect the rights of non-smokers are now sweeping the globe. Can a dog's life-span be cut in half by a smoking master? Would you intentionally double the risk of heart attack or triple the risk of lung cancer for a spouse or family member? Why kill the innocent too? Are non-smokers who get extremely upset at having to breathe side-stream smoke simply being obnoxious or are they fighting to protect themselves and those they love from the known harms generated from burning a plant that contains 44 known cancer causing agents and releases 4,000+ chemical compounds when burned? Do you know a child whose mother smoked while pregnant, who does not suffer from some form of impairment today? Look closely. OUR LIE: Quitting causes weight gain and it's just as dangerous. THE TRUTH: This intellectual denial pre-assumes a large weight gain and then makes an erroneous judgment regarding relative risks. Quitting does not increase our weight, eating does. Some assert that metabolic changes associated primarily with the heart not having to work as hard could account for a pound or two but as far as being " dangerous," you'd have to gain at least 75 additional pounds in order to equal the health risks associated with smoking one pack a day. Keep in mind that your general health, physical abilities and lung capacity will all improve dramatically. If patient, you will soon regain the ability to build cardiovascular endurance, and experience up to a 30% increase in overall lung function within 90 days. You'll be able to apply the same mental recovery tools needed to take control of your addiction in shedding any extra pounds, just one pound at a time. Remember, smoking was your cue that a meal had ended. Unless you develop a new healthy cue there may be fewer leftovers. Also keep in mind how easy it would be for a drug addict to use intentional weight gain to a ploy to sabotage recovery. Additionally, nicotine stimulated brain dopamine pathways and so does food. Be careful not to use food as a destructive dopamine replacement crutch. If at all concerned, consider having a supply of fresh fruits and veggies cut up, handy and ready to eat during the 2-3 weeks it takes the brain to restore natural dopamine pathway sensitivities. OUR LIE: It's too late now to heal these lungs. THE TRUTH: Nonsense! While true that each and every puff destroyed more of each lung's roughly 300 million air sacs (alveoli), we were each blessed with millions more than needed to live a full and complete life. It's amazing how much damaged lungs can repair themselves unless disease or cancer has already arrived. Even with emphysema, although destroyed air sacks will never again function, quitting now will immediately halt the needless destruction of additional sacs. You only have two options - decay or heal, including the possibility of experiencing up to a 30 percent increase in overall lung function within 90 days of quitting. If continuing assault by the 81 cancer causing chemicals so far identified in cigarette smoke, which cigarette in which pack contains the spark that gives birth to that first cancerous cell? OUR LIE: I'd quit but withdrawal never ends! THE TRUTH: Hogwash! If you remain 100% nicotine free for just 72 hours your blood will become nicotine free, your withdrawal anxieties will peak in intensity and the number of psychological craves will peak in number. The greatest challenge will be over. Actual physical withdrawal will be complete within 2-3 weeks as the brain re-sensitizes dopamine pathway receptors and down-regulates their numbers to levels seen in non-smokers. During that time you'll encounter and recondition (extinguish) all but remote or seasonal psychological habit crave triggers and begin to witness the gradually diminishing influence of thousands of nicotine replenishment memories, memories that belonged to an actively feeding addict who once again was in need of a fix. If you focus on taking recovery just one hour, challenge and day at a time, before you know it you'll experience your first day of total comfort, where never once do you think about wanting to smoke nicotine. I call it a silent celebration because you probably won't even realize that it has happened until the next day. After the first such day, they grow more and more frequent until they become your new sense of normal. If just starting out, the rich and deep sense of comfort and calm that awaits you is beyond your enslaved mind's ability to comprehension. Why? Because your dopamine pathways, your mind's priorities teacher, have been hijacked, making that next nicotine fix as important as eating food. Food craves, nicotine craves but with one critical difference. Without food we die. Without nicotine we thrive. It's why, although as real as your name, you cannot trust the nicotine wanting message that pounds inside your head, as it is false and is destroying you. OUR LIE: But the craves last for hours! THE TRUTH: Just like the lingering thought of a nice juicy steak, lobster in butter sauce, or fresh baked hot apple pie, you can make yourself "think" about having a cigarette all day long, if that's what you really want to do. Unlike fixating on a conscious thought about smoking, subconsciously cue triggered crave anxiety attacks almost always last for less than 3 minutes. But it's important that you look at a clock and time the crave episode as cessation time distortion (a normal and expected recovery symptom) can make minutes feel like hours. The good news is that most of the anxiety surrounding crave episodes is self induced and thus controllable. Key is in not trying to hide or run from your mind's junkie thinking but exposing it to honest analysis and positive thinking. Strip away all the self-inflicted anxiety and at worst, what remains on quitting day 3 for the "average" quitter is just 18 minutes of true crave anxiety (an average of six craves, each less than three minutes in duration). OUR LIE: I'll quit after the next pack, next carton, next month, my next birthday or New Years. THE TRUTH: Oh really? Can you count on both hands and all your toes how many times you've lied to yourself with such nonsense? And which pack, carton, month or birthday will give you the best chance for success? Forget buying nicotine laden cigarettes by the pack or carton. A case is even cheaper! With the way that cigarette prices are shooting through the roof, you might as well calculate how many it will take to keep you in nicotine for life and buy them all now. The only problem with that is in determining how long you have left to live. How many more pack, carton, birthday and New Year's lies will you tell to yourself? When will they stop? If you continue on your present path, many Birthdays will likely be canceled by a rather early Deathday. You are a true drug addict in every sense and the "wanting" inside your brain is as real as the greatest truth you know. What isn't true is the message, that that next fix is important. Truth is, everything now done under nicotine's influence can be done as well as or better without it. OUR LIE: I like to smoke when I drink and I find myself smoking even more. THE TRUTH: The effects of drinking and stress upon our body's nicotine level are nearly the same. You smoke more when you drink not because you "like" to but because you MUST. Like stress, alcohol is an acid producing event that causes urine to become more acidic. The greater the acid level of urine, the quicker our kidneys remove and eliminate nicotine reserves from the bloodstream. Thus, the more you drink, the more nicotine you'll need to smoke or ingest in order to avoid sensing the onset of the anxiety of early withdrawal. Although early alcohol use contributes to destroying a great many quit attempts, understanding the nicotine-acid relationship can be of benefit in accelerating physical nicotine withdrawal so that quitters can begin feeling relief sooner. Acidic fruit juices, such as cranberry, may help reduce the normal 72 hours of withdrawal required to remove all nicotine from the blood. In that roughly 50% of all relapses are associated with alcohol use, if at all possible don't drink during the first few days of recovery. When you do decide to drink, consider drinking at home first without cigarettes around before testing your resolve around smokers. By doing so you'll help to break the your mind's psychological links between smoking and drinking with as little risk as possible. As millions of ex-smokers can attest, your beer or drink will taste better than ever once your taste buds are allowed an opportunity to heal. OUR LIE: It's too painful to quit! THE TRUTH: Compared to what? Three days of physical withdrawal (just 72 hours) in no way compares to the pain of months of chemotherapy, lung removal surgery and a two foot scar, a losing battle with throat cancer, years of trying to recover from a serious stroke or massive heart attack, or fighting for every breath through emphysema riddled lungs as you drag oxygen around for the balance of life. If you're really worried about hurt then why continue your daily destruction? OUR LIE: If I quit, I'll just start back again. I always do. THE TRUTH: The truth is that you do not have to relapse. We relapse because we rewrite the Law of Addiction, we forget why we quit, or we invent lies and stupid excuses, such as those that fill this page. Your next quit can be your last but you need to learn how to care for your recovery, while always applying the only rule that you'll ever need to obey - to NEVER TAKE ANOTHER PUFF! OUR LIE: I'll cut down or quit and smoke just one now and then. THE TRUTH: It's every addict's dream, to control the uncontrollable. You are addicted to a substance that is five times as addictive as powdered cocaine (15% vs. 75%). You may be strong enough to cut back but so long as nicotine continues to arrive you'll remain hooked, the decay will continue, and as studies suggest, even though smoking less your health risks will remain almost unchanged. If you were a pack-a-day nicotine smoker and after quitting you decide to smoke just one cigarette, you might as well get ready to smoke the other 7,300 for the year too as full and complete relapse is virtually assured. The Law of Addiction is simple - just one puff of new nicotine and it's over. Brain scans show that up to 50% of dopamine pathway receptors become occupied by nicotine within eight seconds of the first puff. While roughly half walk away from relapse totally convinced that they've gotten away with smoking just once, they've saturated and de-sensitized dopamine pathway receptors and will soon find their brain begging for more. You see, as permanent as alcoholism, once hooked we somehow stay hard wired for relapse for the balance of life. Although recovery allows the brain time to heal and function normally again the tracks of addiction remain. We cannot cure or kill our disease. Once free, we remain on probation for the balance of life. OUR LIE: I tried quitting but my family stopped supporting me or was giving me such a hard time that it caused me to throw in the towel. THE TRUTH: It's a lie. You gave up because you used your family as a cheap excuse to get your drug back. You exaggerated everything they did or didn't do. You were looking for any excuse. You're the drug addict yet you expected them to understand the weakness and thinking of a drug addict's mind. Maybe they didn't pat you on the back as often as you wanted, but is it really fair to expect them to appreciate the magnitude or duration of your challenge if they've never been through chemical withdrawal themselves? They just want you to be normal. They don't know how to react. Do they pat you on the back and keep reminding you, or hope and pray that the worst has already passed? Feeling unappreciated, picking fights and creating confrontation are tools of the addict's mind that are often used as weapons in order to reclaim their drug. Some know that if they inflict tremendous stress on loved ones that they may even convince their loved one to beg them to start smoking nicotine again, or better yet, to go buy their relapse cigarettes for them. That way, they can blame their relapse on their loved one. "They just couldn't handle my quitting." "Maybe next time!" The lengths to which we'll go in order to feed our wanting are almost beyond belief. Yes, some of us will even hurt those that love us most. OUR LIE: OK, I'm going to stop! Now I can enjoy my smokes until then! THE TRUTH: If you've done this more than once, isn't it just more junkie head games? This addict wants to feel good about smoking nicotine and they've learned that by saying that they're going to quit, that they make themselves feel better even though deep down they know that it's probably just another lie! Unless something awakens this addict, there may never be a serious quit in their future. OUR LIE: I've got to die of something! THE TRUTH: True, but if you knew that tomorrow morning at 9:22 a.m. a massive smoking induced stroke would bring your life to an abrupt end, and you'd die on a cold floor with a cigarette beside you - just as tens of thousands of smokers are found each year? Would you light that last cigarette at 9:21 a.m. and pull the trigger that kills you? Is this one of your primary use rationalizations? Look around at all the smokers you see today. The death certificates of half will read, "cause of death - smoking." Yes, they had to die of something but not an average of more than 5,000 days early. Have you met Noni, Bryan, Deb and Kim? Would any non-addicted human spend each and every day of the remainder of their life intentionally destroying more of their body's ability to receive and transport life giving oxygen? Would they continue doing so until physical exercise was no longer an option, or until this mental illness called dependency forced others to begin caring for us, as they watch us struggle just to suck oxygen from tanks and machines? Which family member have you prepared to be your care giver? Try to imagine what it's like to breathe through a straw? It's called emphysema. Why not find a straw and give it a try. What has nicotine done for you lately? OUR LIE: I can't quit alone. I'll need nicotine gum, the patch, hypnosis, e-cigs, acupuncture, magic herbs or other wonder drugs! THE TRUTH: Wrong! The simple truth is that no magic cure has ever "made" any smoker quit smoking nicotine. The key to immediate and lasting abstinence is education and understanding, in becoming vastly more dependency recovery savvy than our addiction is strong. Hypnosis and acupuncture teach us nothing, nor does use of nicotine replacement products that fail roughly 93% of users within 6 months of quitting, while making NRT slaves of a substantial percentage of those who actually quit smokings. What quitting product and procedure salesmen will never tell you is that each year cold turkey generates more successful long-term ex-users than all other quitting methods combined. Why? Because they want your money. Remember, should all else fail, you always have you! OUR LIE: It's all Nicodemon's fault, not mine! THE TRUTH: There is no Nicodemon, no little monsters, no big monsters, no monsters at all. None! In fact, the title to this article, Nicodemon's Lies, is one of the biggest lies of all. They were never Nicodemon's lies but our lies. Nicotine is simply a chemical, a drug, an alkaloid known as C10H14N2. Its I.Q. is and always has been zero. It does not think, plan, inflict punishment, nor will it conspire to make you relapse or die addicted to it. The fact that it has zero intelligence has always been your greatest weapon. Everything you see, feel, and sense during nicotine withdrawal and recovery will be grounded in chemical dependency, conditioning, reason, logic, emotion or science. Any conspirators in any past attempts to make you relapse and destroy your recovery were always and only "you!" Never once did you relapse due to external circumstances. It was 100% internal, once again you introduced nicotine into your bloodstream. The good news is that while each defeat was yours, so too will be the victory. Should you end nicotine's control of your brain's reward pathways the victory will belong only to you!